

Primary-Sjögren's-Syndrome-Related Interstitial Lung Disease: A Clinical Review Discussing Current Controversies
- PMID: 37240535
- PMCID: PMC10218845
- DOI: 10.3390/jcm12103428
Primary-Sjögren's-Syndrome-Related Interstitial Lung Disease: A Clinical Review Discussing Current Controversies
Abstract
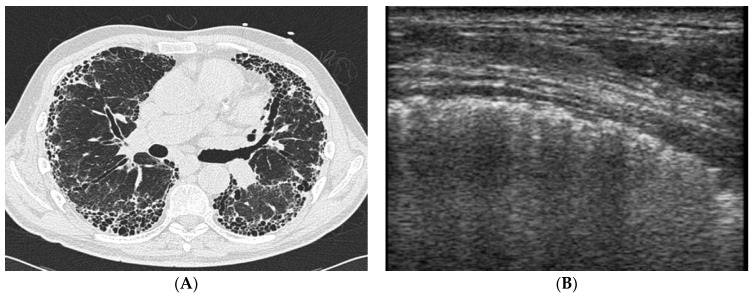
Lung involvement, especially interstitial lung disease, is a potentially severe extra-glandular manifestation of Primary Sjogren's Syndrome (pSS-ILD). ILD can manifest either as a late complication of pSS or anticipate sicca symptoms, likely reflecting two different patho-physiological entities. Presence of lung involvement in pSS subjects can remain subclinical for a long time; therefore, patients should be actively screened, and lung ultrasound is currently being investigated as a potential low cost, radiation-free, easily repeatable screening tool for detection of ILD. In contrast, rheumatologic evaluation, serology testing, and minor salivary gland biopsy are crucial for the recognition of pSS in apparently idiopathic ILD patients. Whether the HRCT pattern influences prognosis and treatment response in pSS-ILD is not clear; a UIP pattern associated with a worse prognosis in some studies, but not in others. Many aspects of pSS-ILD, including its actual prevalence, association with specific clinical-serological characteristics, and prognosis, are still debated by the current literature, likely due to poor phenotypic stratification of patients in clinical studies. In the present review, we critically discuss these and other clinically relevant "hot topics" in pSS-ILD. More specifically, after a focused discussion, we compiled a list of questions regarding pSS-ILD that, in our opinion, are not easily answered by the available literature. We subsequently tried to formulate adequate answers on the basis of an extensive literature search and our clinical experience. At the same, we highlighted different issues that require further investigation.
Keywords: Sjögren’s; interstitial lung disease; lung ultrasound; patterns; prognosis; treatment.
Conflict of interest statement
G.S. received honoraria from Boehringer Ingelheim outside of the submitted work. The remaining authors declare no relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Ramos-Casals M., Brito-Zerón P., Seror R., Bootsma H., Bowman S.J., Dörner T., Gottenberg J.E., Mariette X., Theander E., Bombardieri S., et al. Characterization of systemic disease in primary Sjögren’s syndrome: EULAR-SS Task Force recommendations for articular, cutaneous, pulmonary and renal involvements. Rheumatology. 2015;54:2230–2238. doi: 10.1093/rheumatology/kev200. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
