

Adverse childhood experiences and adolescent cannabis use trajectories: findings from a longitudinal UK birth cohort
- PMID: 37244674
- PMCID: PMC10751739
- DOI: 10.1016/S2468-2667(23)00095-6
Adverse childhood experiences and adolescent cannabis use trajectories: findings from a longitudinal UK birth cohort
Abstract
Background: Adverse childhood experiences (ACEs) are classically defined as physical abuse, sexual abuse, emotional abuse, emotional neglect, bullying, parental substance use or abuse, violence between parents, parental mental health problems or suicide, parental separation, or a parent convicted of criminal offence. Exposure to ACEs can be associated with cannabis use, but no comparisons across all adversities have been made while also considering timing and frequency of cannabis use. We aimed to explore the association between ACEs and cannabis use timing and frequency in adolescence, considering the cumulative number of ACEs and individual ACEs.
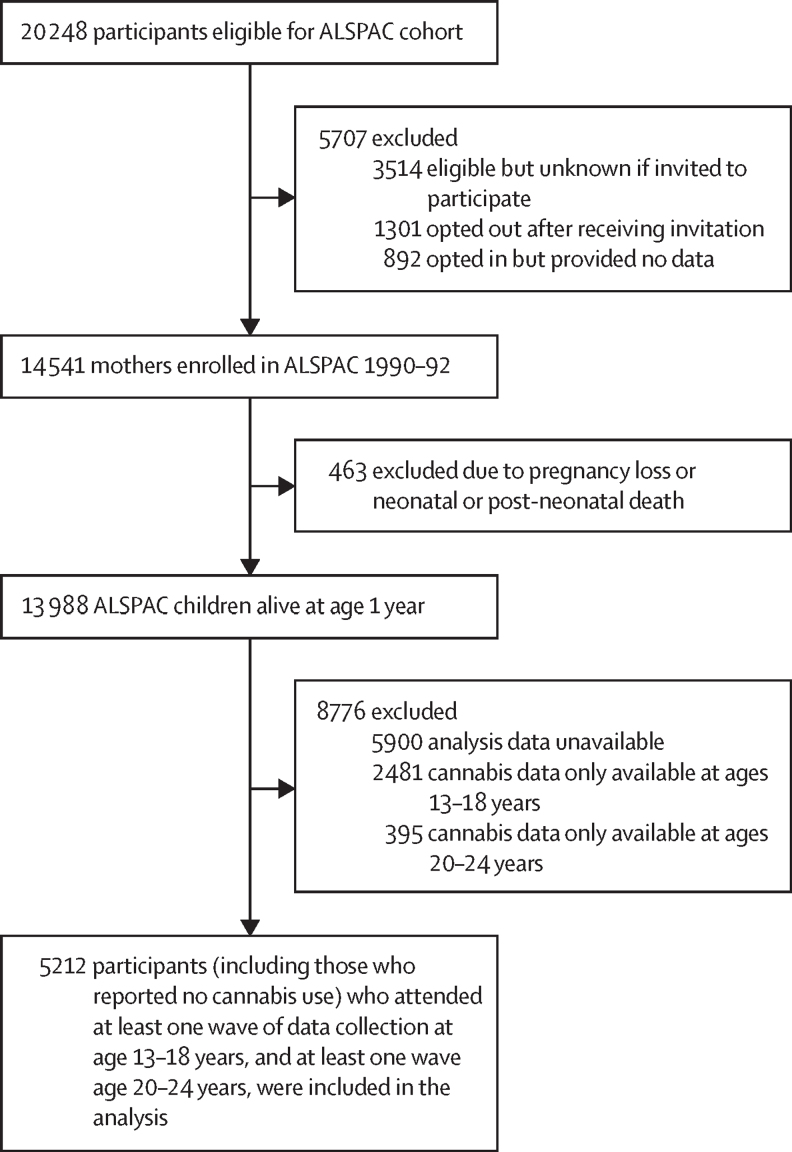
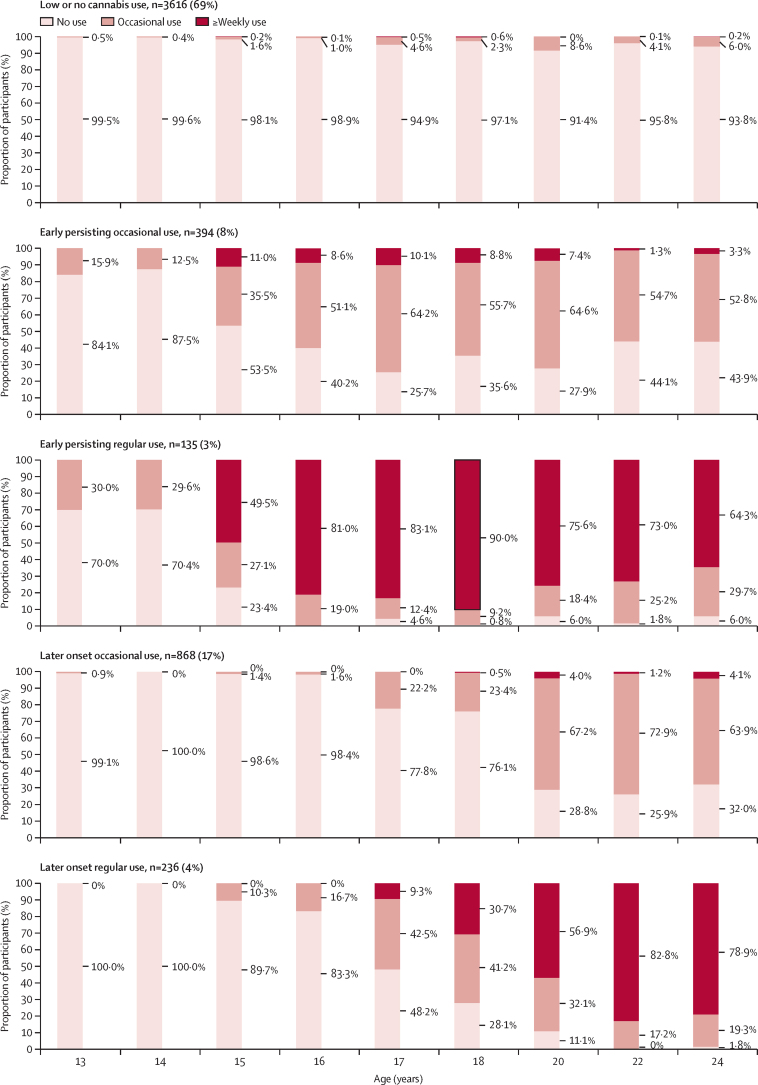
Methods: We used data from the Avon Longitudinal Study of Parents and Children, a longitudinal UK birth cohort study. Longitudinal latent classes of cannabis use frequency were derived from self-reported data at multiple timepoints in participants aged 13-24 years. ACEs between ages 0 years and 12 years were derived from prospective and retrospective reports at multiple timepoints by parents and the participant. Multinomial regression was used to analyse the effect of both cumulative exposure to all ACEs and the ten individual ACEs on cannabis use outcomes.
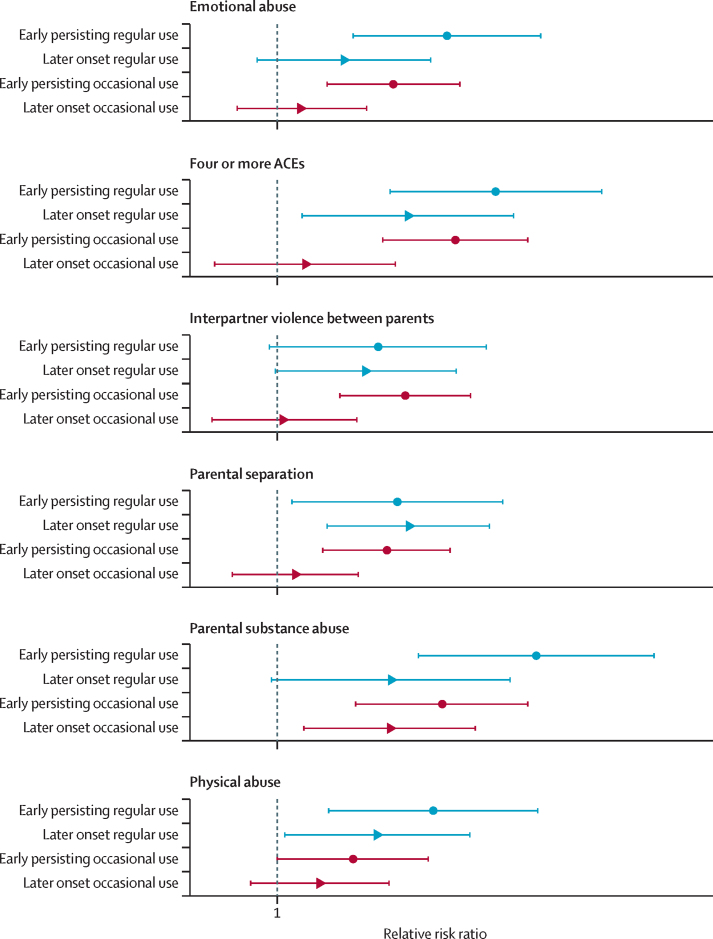
Findings: 5212 participants (3132 [60·0%] were female and 2080 [40·0%] were male; 5044 [96·0%] were White and 168 [4·0%] were Black, Asian, or minority ethnic) were included in this study. After adjustment for polygenic risk and environmental risk factors, participants who had 4 or more ACEs at age 0-12 years were at increased risk of early persisting regular cannabis use (relative risk ratio [RRR] 3·15 [95% CI 1·81-5·50]), later onset regular use (1·99 [1·14-3·74]), and early persisting occasional use (2·55 [1·74-3·73]) compared with low or no cannabis use. After adjustment, early persisting regular use was associated with parental substance use or abuse (RRR 3·90 [95% CI 2·10-7·24]), parental mental health problems (2·02 [1·26-3·24]), physical abuse (2·27 [1·31-3·98]), emotional abuse (2·44 [1·49-3·99]), and parental separation (1·88 [1·08-3·27]) compared with low or no cannabis use.
Interpretation: Risks for problematic adolescent cannabis use are highest for individuals reporting 4 or more ACEs, and were particularly raised for those with parental substance use or abuse. Public health measures to address ACEs might reduce adolescent cannabis use.
Funding: The Wellcome Trust, UK Medical Research Council, Alcohol Research UK.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests ML is employed by Drug Science, which receives an unrestricted educational grant from a consortium of medical cannabis companies to further its mission, that is the pursuit of an unbiased and scientific assessment of drugs regardless of their regulatory class. All other authors declare no competing interests.
Figures
Similar articles
-
Associations of adverse childhood experiences with educational attainment and adolescent health and the role of family and socioeconomic factors: A prospective cohort study in the UK.PLoS Med. 2020 Mar 2;17(3):e1003031. doi: 10.1371/journal.pmed.1003031. eCollection 2020 Mar. PLoS Med. 2020. PMID: 32119668 Free PMC article.
-
Adverse childhood experiences and early life inflammation in the Avon longitudinal study of parents and children.Psychoneuroendocrinology. 2020 Dec;122:104914. doi: 10.1016/j.psyneuen.2020.104914. Epub 2020 Oct 13. Psychoneuroendocrinology. 2020. PMID: 33129041 Free PMC article.
-
The association between poverty and longitudinal patterns of adverse childhood experiences across childhood and adolescence: Findings from a prospective population-based cohort study in the UK.Child Abuse Negl. 2024 Oct;156:107014. doi: 10.1016/j.chiabu.2024.107014. Epub 2024 Sep 4. Child Abuse Negl. 2024. PMID: 39232377
-
Adverse Childhood Experiences Are Associated with Mental Health Problems Later in Life: An Umbrella Review of Systematic Review and Meta-Analysis.Neuropsychobiology. 2025;84(1):48-64. doi: 10.1159/000542392. Epub 2024 Nov 18. Neuropsychobiology. 2025. PMID: 39557030
-
Is parental unemployment associated with increased risk of adverse childhood experiences? A systematic review and meta-analysis.J Public Health (Oxf). 2023 Nov 29;45(4):829-839. doi: 10.1093/pubmed/fdad069. J Public Health (Oxf). 2023. PMID: 37253685 Free PMC article.
Cited by
-
Associations of childhood adversity and substance use disorder polygenic scores with disorder severity and diagnostic criteria.Psychol Med. 2025 May 2;55:e132. doi: 10.1017/S0033291725001163. Psychol Med. 2025. PMID: 40314172 Free PMC article.
-
Childhood Sexual Trauma, Substance Use, and Antiretroviral Therapy Adherence Among Older Adults Living With HIV: A Mediational Analysis.J Appl Gerontol. 2025 Feb;44(2):222-230. doi: 10.1177/07334648241271903. Epub 2024 Sep 24. J Appl Gerontol. 2025. PMID: 39316826 Free PMC article.
-
Examining the Interactive Associations of Cannabis and Alcohol Outlets With Self-harm Injuries in California: A Spatiotemporal Analysis.Epidemiology. 2025 Mar 1;36(2):196-206. doi: 10.1097/EDE.0000000000001822. Epub 2024 Dec 16. Epidemiology. 2025. PMID: 39679582 Free PMC article.
-
Longitudinal study of risk factors predicting cannabis use disorder in UK young adults and adolescents.Commun Med (Lond). 2025 Jul 19;5(1):300. doi: 10.1038/s43856-025-01018-y. Commun Med (Lond). 2025. PMID: 40683963 Free PMC article.
-
The Developmental Trajectory to Cannabis Use Disorder.Am J Psychiatry. 2024 May 1;181(5):353-358. doi: 10.1176/appi.ajp.20231006. Am J Psychiatry. 2024. PMID: 38706340 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
- DH_/Department of Health/United Kingdom
- MC_PC_15018/MRC_/Medical Research Council/United Kingdom
- MR/L022206/1/MRC_/Medical Research Council/United Kingdom
- MR/L010305/1/MRC_/Medical Research Council/United Kingdom
- G9815508/MRC_/Medical Research Council/United Kingdom
- 217065/Z/19/Z/WT_/Wellcome Trust/United Kingdom
- MC_PC_19009/MRC_/Medical Research Council/United Kingdom
- MR/N00616X/1/MRC_/Medical Research Council/United Kingdom
- MR/M020894/1/MRC_/Medical Research Council/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- MR/M006727/1/MRC_/Medical Research Council/United Kingdom
- 209158/Z/17/Z/WT_/Wellcome Trust/United Kingdom
