

Integration of clinical sequencing and immunohistochemistry for the molecular classification of endometrial carcinoma
- PMID: 37245486
- PMCID: PMC10402916
- DOI: 10.1016/j.ygyno.2023.05.059
Integration of clinical sequencing and immunohistochemistry for the molecular classification of endometrial carcinoma
Abstract
Purpose: Using next generation sequencing (NGS), The Cancer Genome Atlas (TCGA) found that endometrial carcinomas (ECs) fall under one of four molecular subtypes, and a POLE mutation status, mismatch repair (MMR) and p53 immunohistochemistry (IHC)-based surrogate has been developed. We sought to retrospectively classify and characterize a large series of unselected ECs that were prospectively subjected to clinical sequencing by utilizing clinical molecular and IHC data.
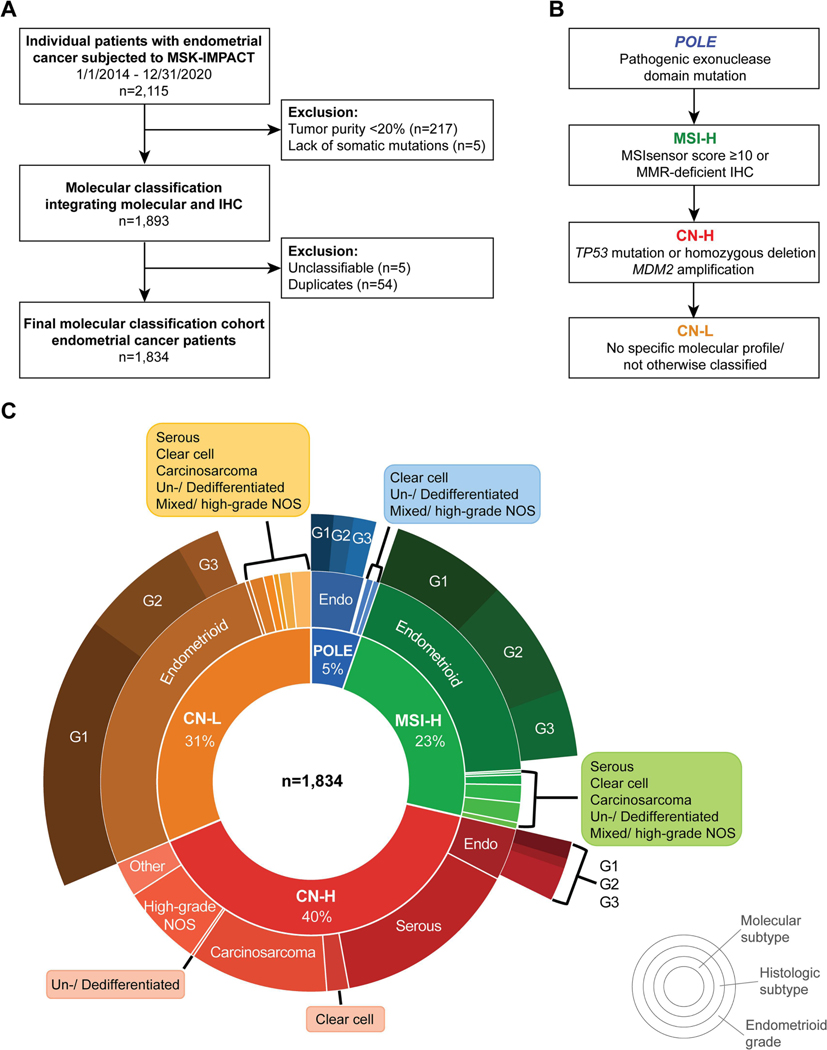
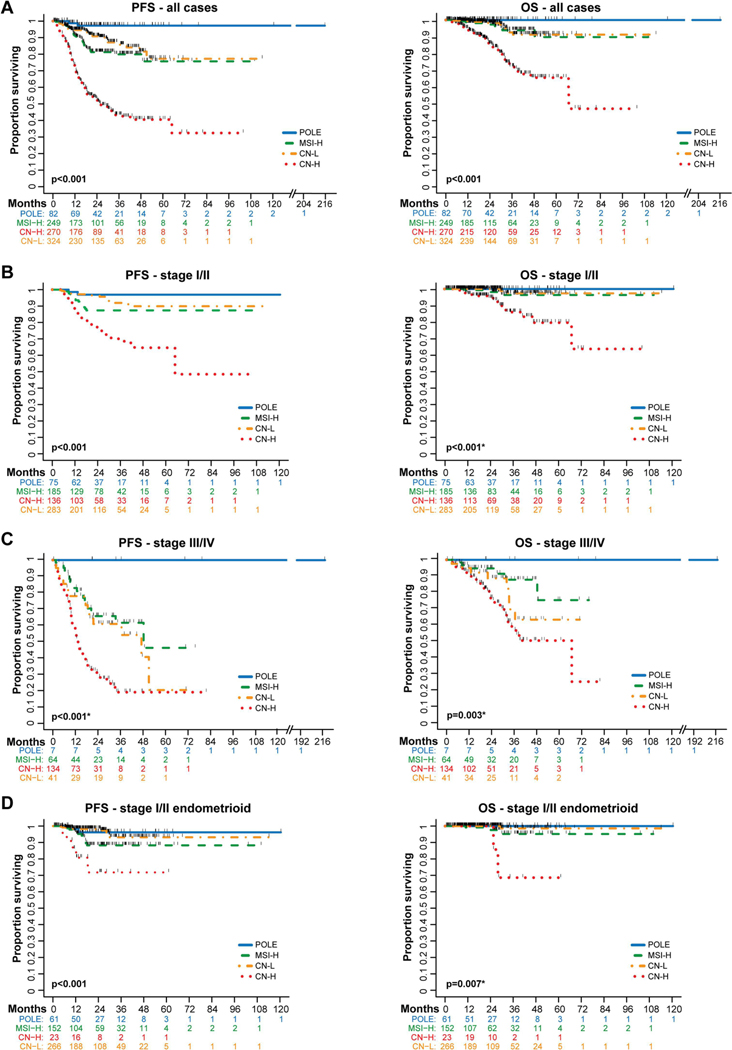
Experimental design: All patients with EC with clinical tumor-normal MSK-IMPACT NGS from 2014 to 2020 (n = 2115) were classified by integrating molecular data (i.e., POLE mutation, TP53 mutation, MSIsensor score) and MMR and p53 IHC results. Survival analysis was performed for primary EC patients with upfront surgery at our institution.
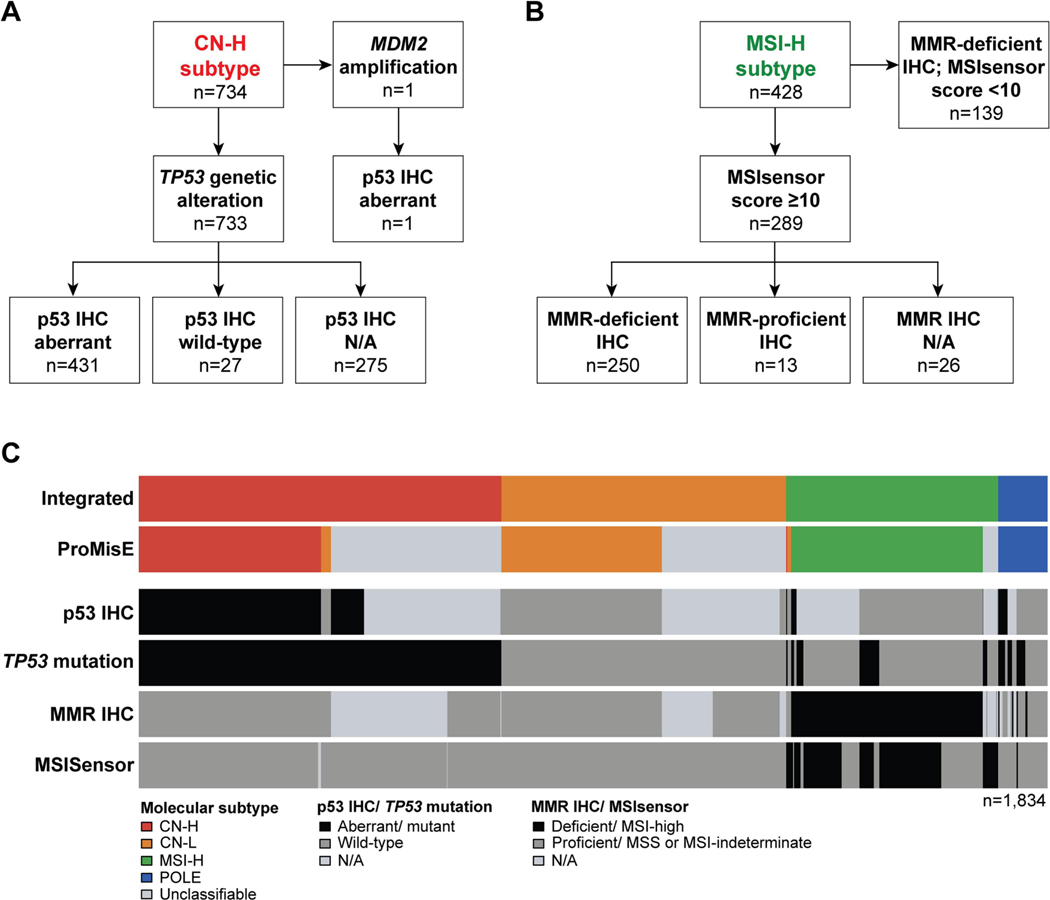
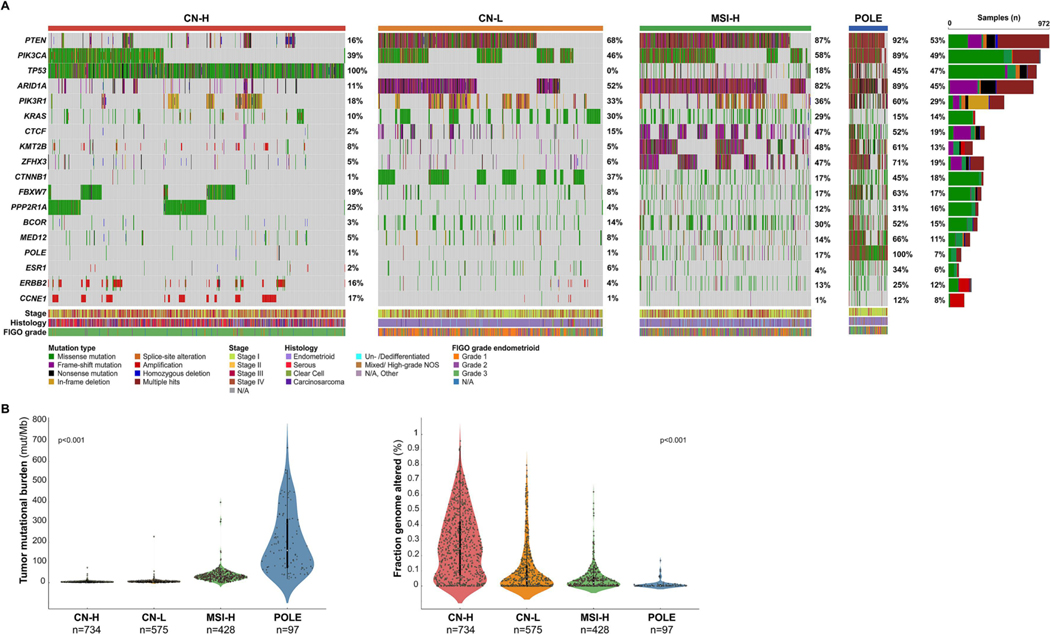
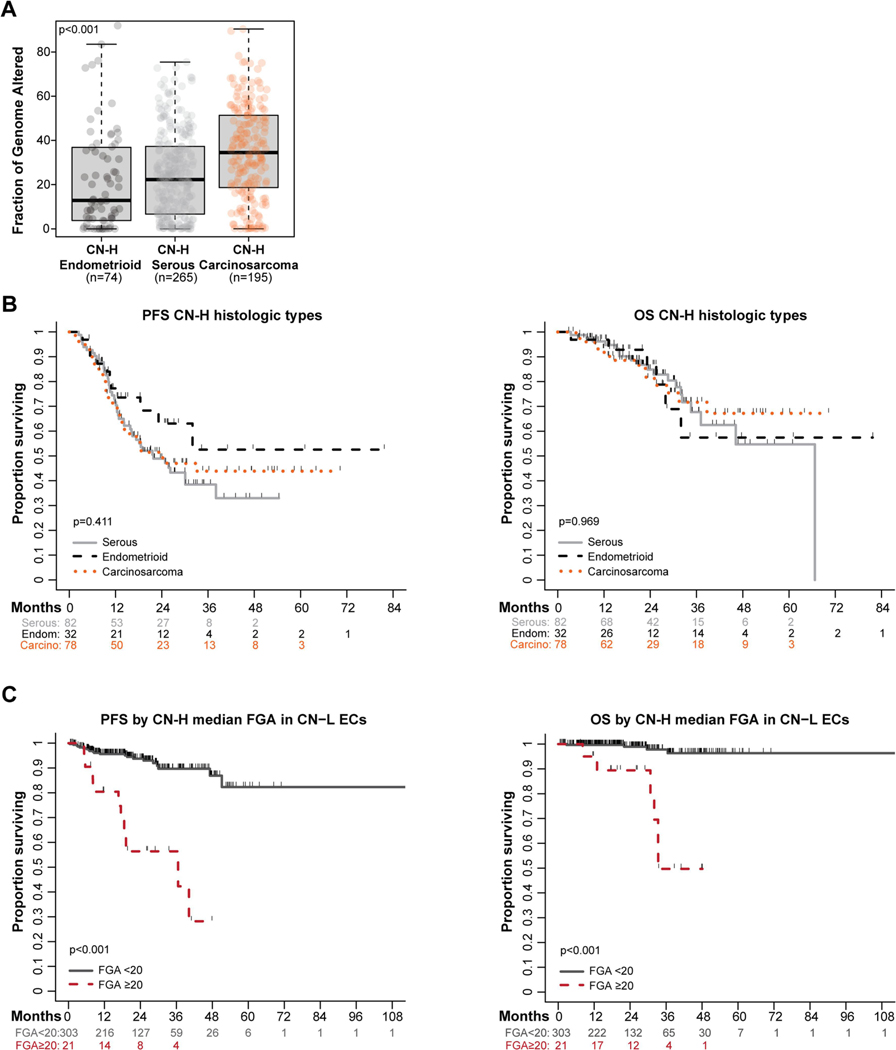
Results: Utilizing our integrated approach, significantly more ECs were molecularly classified (1834/2115, 87%) as compared to the surrogate (1387/2115, 66%, p < 0.001), with an almost perfect agreement for classifiable cases (Kappa 0.962, 95% CI 0.949-0.975). Discrepancies were primarily due to TP53 mutations in p53-IHC-normal ECs. Of the 1834 ECs, most were of copy number (CN)-high molecular subtype (40%), followed by CN-low (32%), MSI-high (23%) and POLE (5%). Histologic and genomic variability was present amongst all molecular subtypes. Molecular classification was prognostic in early- and advanced-stage disease, including early-stage endometrioid EC.
Conclusions: The integration of clinical NGS and IHC data allows for an algorithmic approach to molecularly classifying newly diagnosed EC, while overcoming issues of IHC-based genetic alteration detection. Such integrated approach will be important moving forward given the prognostic and potentially predictive information afforded by this classification.
Keywords: Clinical sequencing; Endometrial carcinoma; Immunohistochemistry; Molecular classification; Mutation.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest N.R. Abu-Rustum reports Stryker/Novadaq and GRAIL grants paid to the institution, outside the current study. C.F. Friedman reports institutional research support from Seagen, Merck, BMS, AstraZeneca, Mersana and Hotspot Therapeutics; consulting fees from BMS, Seagen and Aadi Biosciences; honoraria for lectures from Onclive; meeting/ travel support by Puma; participation on Data Safety Monitoring or Advisory Board of Merck, Genentech and Marengo (all uncompensated). D. Zamarin reports institutional research support from AstraZeneca, Merck, Plexxikon Synthekine and Genentech; consulting fees from AstraZeneca, Synthekine, Astellas, Tessa Therapeutics, Memgen, Celldex, Crown Biosciences, Hookipa Biotech, Kalivir, Xencor and GSK; royalties from Merck; and stock options from Accurius Therapeutics, ImmunOS Therapeutics and Calidi Biotherapeutics, all outside the submitted work. V. Makker reports meeting/travel support by Eisai and Merck; participation on Data Safety Monitoring or Advisory Board of Duality, Merck, Karyopharm, Exelexis, Eisai, Karyopharm, BMS, Clovis, Faeth Immunocore, Morphosys, AstraZeneca, Novartis, GSK, Bayer (all unpaid), and study support to the institution by Merck, Eisai, AztraZeneca, Faeth, Karyopharm, Zymeworks, Duality, Clovis, Bayer and Takeda. Y. Liu reports institutional research funding from Repare Therapeutics, AstraZeneca and GSK; honoraria from Total Health and Sarah Lawrence College; and travel/meeting support by AstraZeneca, outside the submitted work. B. Weigelt reports a research grant from REPARE Therapeutics paid to the institution, outside the submitted work. D.S. Chi reports personal fees from Apyx Medical, Verthermia Inc., Biom ‘Up, and AstraZeneca, as well as recent or current stock/options ownership of Apyx Medical, Verthemia, Intuitive Surgical, Inc., TransEnterix, Inc., Doximity, Moderna, and BioNTech SE. E.L. Jewell reports personal fees from Covidien/Medtronic. M. M. Leitao is an ad hoc speaker for Intuitive Surgical, Inc.; outside the submitted work, he is on the Advisory Board of Ethicon/Johnson & Johnson and Takeda; and reports grants paid to the institution by KCI/Acelity. C. Aghajanian reports clinical trial funding paid to the institution from AstraZeneca; consulting fees (advisory board) from Eisai/Merck, Roche/Genentech, Abbvie, AstraZeneca/Merck, and Repare Therapeutics; advisory board participation (no fee) for Blueprint Medicine; and leadership/fiduciary roles for the GOG Foundation Board of Directors (travel cost reimbursement) and NRG Oncology Board of Directors (unpaid). The remaining authors have no conflicts of interest to declare.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71:209–49. - PubMed
-
- Murali R, Soslow RA, Weigelt B. Classification of endometrial carcinoma: more than two types. Lancet Oncol. 2014;15:e268–78. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
