Comparative outcomes of acute colonic diverticulitis in immunocompromised versus immunocompetent patients: a systematic review and meta-analysis
- PMID: 37248174
- PMCID: PMC10626017
- DOI: 10.5217/ir.2023.00005
Comparative outcomes of acute colonic diverticulitis in immunocompromised versus immunocompetent patients: a systematic review and meta-analysis
Abstract
Background/aims: Immunocompromised patients with acute colonic diverticulitis are at high risk for complications and failure of non-surgical treatment. However, evidence on the comparative outcomes of immunocompromised and immunocompetent patients with diverticulitis is lacking. This systematic review and meta-analysis investigated the outcomes of medical treatment in immunocompromised and immunocompetent patients with diverticulitis.
Methods: A comprehensive literature search was conducted in PubMed, Embase, and the Cochrane Library. Studies comparing the clinical outcomes of immunocompromised and immunocompetent patients with diverticulitis were included.
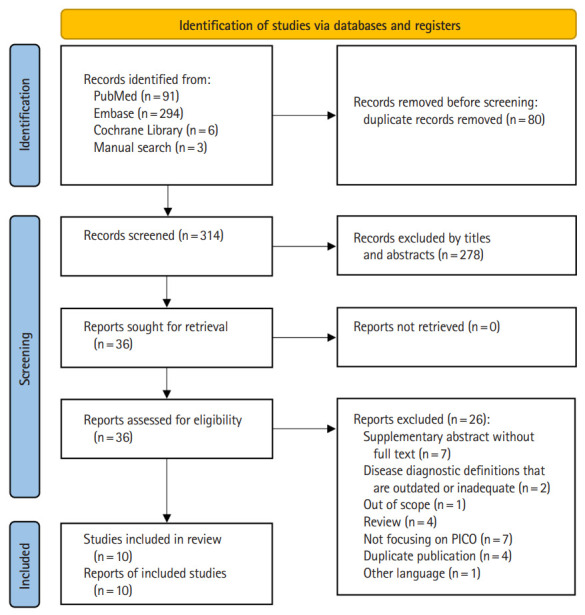
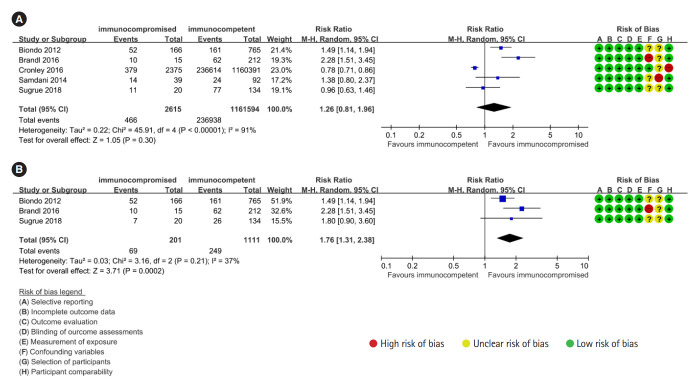
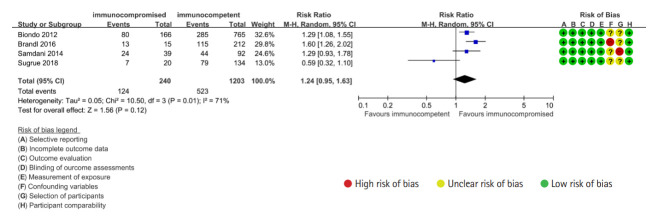
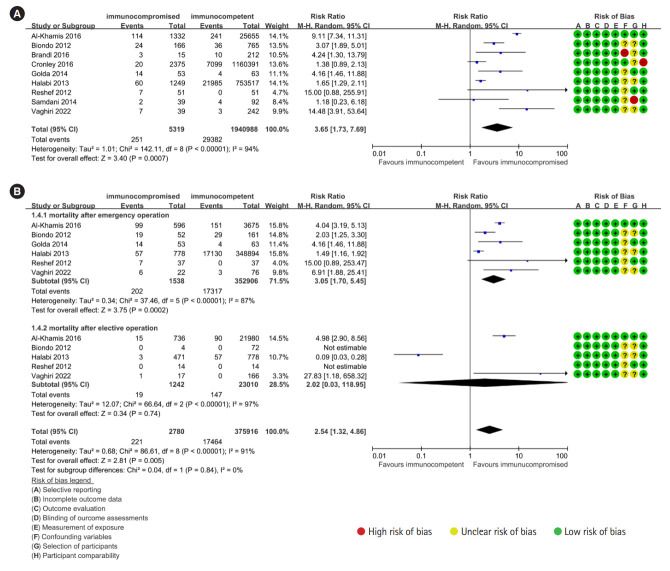
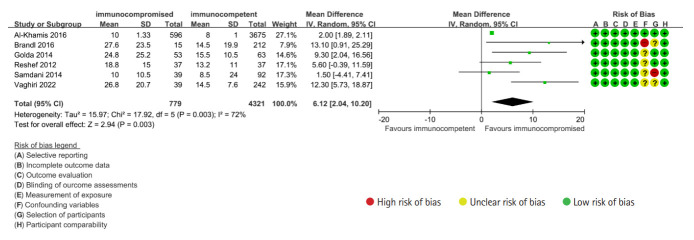
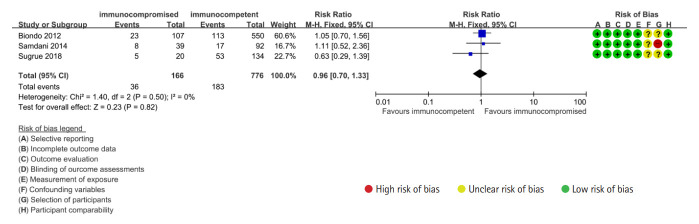
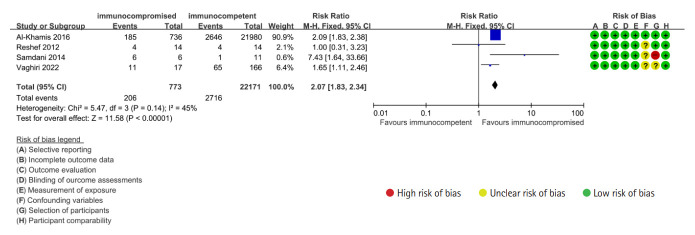
Results: A total of 10 studies with 1,946,461 subjects were included in the quantitative synthesis. The risk of emergency surgery and postoperative mortality after emergency surgery was significantly higher in immunocompromised patients than in immunocompetent patients with diverticulitis (risk ratio [RR], 1.76; 95% confidence interval [CI], 1.31-2.38 and RR, 3.05; 95% CI, 1.70-5.45, respectively). Overall risk of complications associated with diverticulitis was non-significantly higher in immunocompromised than in immunocompetent patients (RR, 1.24; 95% CI, 0.95-1.63). Overall mortality irrespective of surgery was significantly higher in immunocompromised than in immunocompetent patients with diverticulitis (RR, 3.65; 95% CI, 1.73-7.69). By contrast, postoperative mortality after elective surgery was not significantly different between immunocompromised and immunocompetent patients with diverticulitis. In subgroup analysis, the risk of emergency surgery and recurrence was significantly higher in immunocompromised patients with complicated diverticulitis, whereas no significant difference was shown in mild disease.
Conclusions: Immunocompromised patients with diverticulitis should be given the best medical treatment with multidisciplinary approach because they had increased risks of surgery, postoperative morbidity, and mortality than immunocompetent patients.
Keywords: Colonic diverticulitis; Immunocompromised host; Treatment outcome.
Conflict of interest statement
Park YE, Chang JY, and Kim DK are editorial board members of the journal but were not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Figures
Similar articles
-
Acute diverticulitis in immunocompromised patients: evidence from an international multicenter observational registry (Web-based International Register of Emergency Surgery and Trauma, Wires-T).Tech Coloproctol. 2023 Sep;27(9):747-757. doi: 10.1007/s10151-023-02758-6. Epub 2023 Feb 7. Tech Coloproctol. 2023. PMID: 36749438 Free PMC article.
-
Case-matched comparison of perioperative outcomes after surgical treatment of sigmoid diverticulitis in solid organ transplant recipients versus immunocompetent patients.Colorectal Dis. 2012 Dec;14(12):1546-52. doi: 10.1111/j.1463-1318.2012.03077.x. Colorectal Dis. 2012. PMID: 22564266
-
Sigmoid Colectomy for Acute Diverticulitis in Immunosuppressed vs Immunocompetent Patients: Outcomes From the ACS-NSQIP Database.Dis Colon Rectum. 2016 Feb;59(2):101-9. doi: 10.1097/DCR.0000000000000513. Dis Colon Rectum. 2016. PMID: 26734967
-
Operative management of colonic diverticular disease in the setting of immunosuppression: A systematic review and meta-analysis.Am J Surg. 2021 Jan;221(1):72-85. doi: 10.1016/j.amjsurg.2020.06.035. Epub 2020 Jul 8. Am J Surg. 2021. PMID: 32814626
-
Elective surgery for conservatively treated acute uncomplicated diverticulitis: a systematic review of postoperative outcomes.Minerva Surg. 2022 Dec;77(6):591-601. doi: 10.23736/S2724-5691.22.09726-X. Minerva Surg. 2022. PMID: 36409040
Cited by
-
Does type II diabetes mellitus increase the morbidity of patients with diverticulitis?Medicine (Baltimore). 2024 Nov 15;103(46):e40567. doi: 10.1097/MD.0000000000040567. Medicine (Baltimore). 2024. PMID: 39560541 Free PMC article.
-
Not all acute colonic diverticulitis follows the same course: a potential risk for immunocompromised individuals.Intest Res. 2023 Oct;21(4):415-417. doi: 10.5217/ir.2023.00142. Epub 2023 Oct 26. Intest Res. 2023. PMID: 37915178 Free PMC article. No abstract available.
References
-
- Humes DJ, Solaymani-Dodaran M, Fleming KM, Simpson J, Spiller RC, West J. A population-based study of perforated diverticular disease incidence and associated mortality. Gastroenterology. 2009;136:1198–1205. - PubMed
-
- Humes DJ, Fleming KM, Spiller RC, West J. Concurrent drug use and the risk of perforated colonic diverticular disease: a population-based case-control study. Gut. 2011;60:219–224. - PubMed
LinkOut - more resources
Full Text Sources