

Propagative α-synuclein seeds as serum biomarkers for synucleinopathies
- PMID: 37248302
- PMCID: PMC10287557
- DOI: 10.1038/s41591-023-02358-9
Propagative α-synuclein seeds as serum biomarkers for synucleinopathies
Erratum in
-
Author Correction: Propagative α-synuclein seeds as serum biomarkers for synucleinopathies.Nat Med. 2025 Feb;31(2):698. doi: 10.1038/s41591-025-03521-0. Nat Med. 2025. PMID: 39856337 Free PMC article. No abstract available.
Abstract
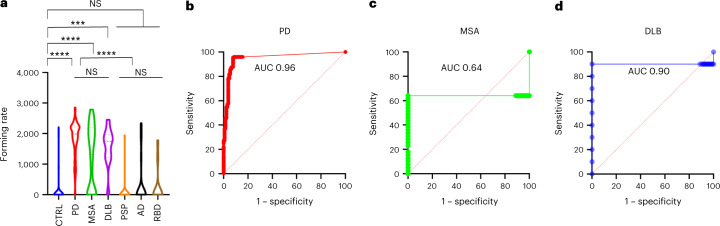
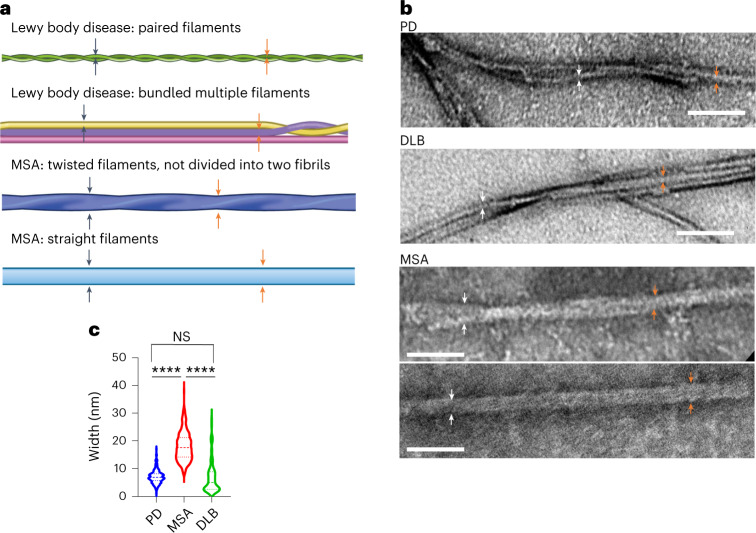
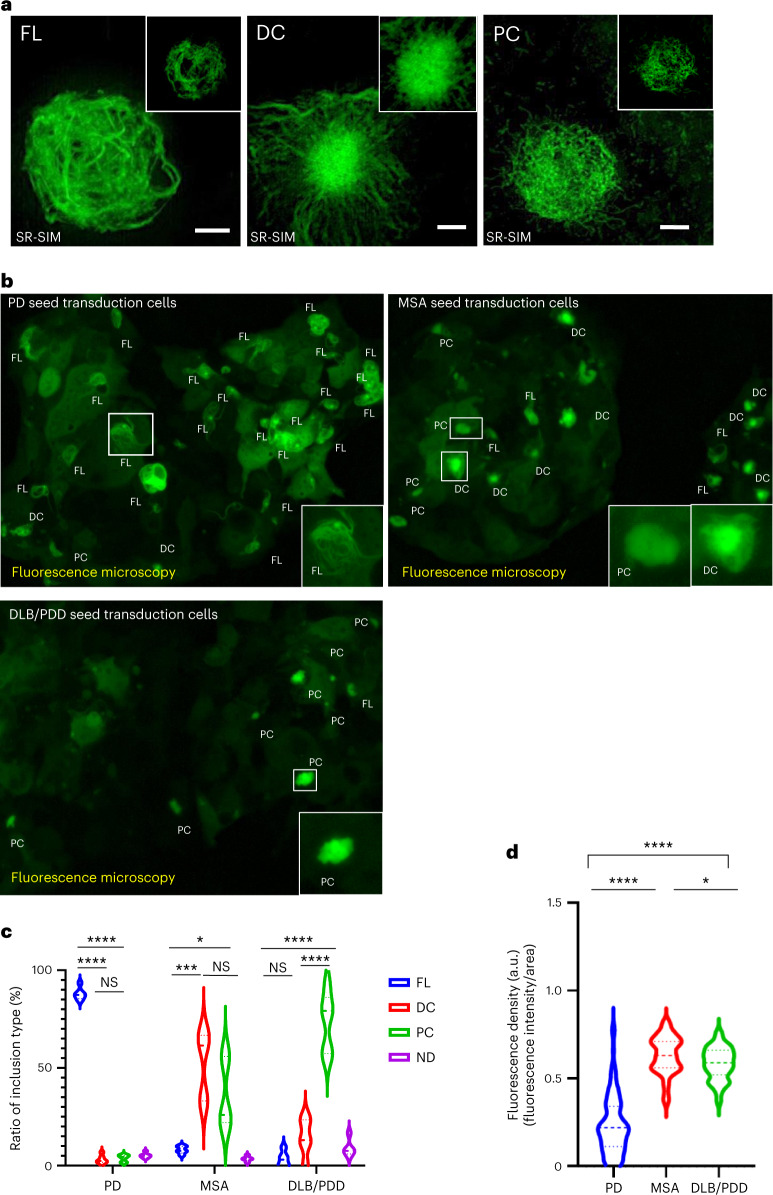
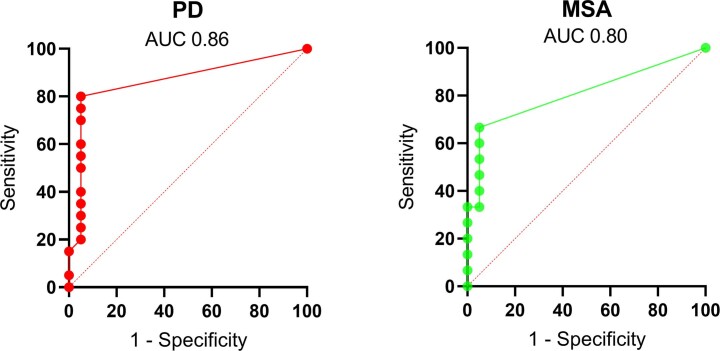
Abnormal α-synuclein aggregation is a key pathological feature of a group of neurodegenerative diseases known as synucleinopathies, which include Parkinson's disease (PD), dementia with Lewy bodies and multiple system atrophy (MSA). The pathogenic β-sheet seed conformation of α-synuclein is found in various tissues, suggesting potential as a biomarker, but few studies have been able to reliably detect these seeds in serum samples. In this study, we developed a modified assay system, called immunoprecipitation-based real-time quaking-induced conversion (IP/RT-QuIC), which enables the detection of pathogenic α-synuclein seeds in the serum of individuals with synucleinopathies. In our internal first and second cohorts, IP/RT-QuIC showed high diagnostic performance for differentiating PD versus controls (area under the curve (AUC): 0.96 (95% confidence interval (CI) 0.95-0.99)/AUC: 0.93 (95% CI 0.84-1.00)) and MSA versus controls (AUC: 0.64 (95% CI 0.49-0.79)/AUC: 0.73 (95% CI 0.49-0.98)). IP/RT-QuIC also showed high diagnostic performance in differentiating individuals with PD (AUC: 0.86 (95% CI 0.74-0.99)) and MSA (AUC: 0.80 (95% CI 0.65-0.97)) from controls in a blinded external cohort. Notably, amplified seeds maintained disease-specific properties, allowing the differentiation of samples from individuals with PD versus MSA. In summary, here we present a novel platform that may allow the detection of individuals with synucleinopathies using serum samples.
© 2023. The Author(s).
Conflict of interest statement
N.H. reports receiving grants and fees unrelated to this research during the conduct of the study; grants from the Japan Society for the Promotion of Science (JSPS), the Japan Agency for Medical Research and Development (AMED), the Japan Science and Technology Agency (JST), the Health and Labour Sciences Research Grant, the International Parkinson and Movement Disorder Society and the Michael J. Fox Foundation for Parkinsonʼs Research; personal fees for speakers honoraria from Sumitomo Pharma, Takeda Pharmaceutical, Kyowa Kirin, AbbVie GK, Otsuka Pharmaceutical, Novartis, Ono Pharmaceutical, Eisai, Teijin Pharma and Daiichi Sankyo; and personal fees for consultancies and advisory boards from Sumitomo Pharma, Takeda Pharmaceutical, Kyowa Kirin, Ono Pharmaceutical, Teijin Pharma and PARKINSON Laboratories. N.H. also owns shares in PARKINSON Laboratories (equity stock (8%)). T.H. reports receiving grants from Kyowa Kirin, the Setsuro Fujii Memorial of the Osaka Foundation for Promotion of Fundamental Medical Research, JSPS KAKENHI (under grant no. 21K07424), the Japan Agency for Medical Research and Development (grant nos. 21wm0425015 and 21dk0207055) and Daiichi Sankyo Selects Research Partners for TaNeDS Collaborative Drug Discovery Project and speakers honoraria from Sumitomo Dainippon Pharma, Takeda Pharmaceutical, Kyowa Kirin, Novartis, Sanofi, Eisai and Otsuka Pharmaceutical during the conduct of the study. A.O. reports receiving grants from the research grant for biogenic amines and neurological disorders and JSPS KAKENHI (under grant no. 19K16928) and speakers honoraria from Takeda Pharmaceutical and Kyowa Kirin, during the conduct of the study. R.K. reports receiving grants and fees unrelated to this research during the conduct of the study; grants from the Fonds National de la Recherche (FNR) Luxembourg, the Fondation Veuve-Metz-Tesch Luxembourg, the Leir Foundation, the Michael J. Fox Foundation for Parkinsonʼs Research (MJFF), the Parkinsonʼs Foundation, the Movement Disorder Society, the European Institute of Innovation and Technology (EIT Health), the Innovative Medicines Initiative (IMI) of the European Union and the European pharmaceutical industry and the European Union’s Horizon 2020 and Horizon Europe research and innovation programs; and personal speaker’s honoraria and/or travel grants from AbbVie, Zambon and Medtronic. R.K. participated as PI or site-PI for industry-sponsored clinical trials without receiving honoraria. The remaining authors declare no competing interests.
Figures

Comment in
-
Blood-Based α-Synuclein Seeding-A New Era for Identifying Parkinsonian Syndromes.Mov Disord. 2023 Aug;38(8):1397-1398. doi: 10.1002/mds.29555. Epub 2023 Jul 25. Mov Disord. 2023. PMID: 37489601 No abstract available.
-
Important advances in movement disorders research in 2023.Lancet Neurol. 2024 Jan;23(1):20-22. doi: 10.1016/S1474-4422(23)00461-1. Lancet Neurol. 2024. PMID: 38101889 No abstract available.
References
-
- Spillantini, M. G. et al. α-Synuclein in Lewy bodies. Nature388, 839–840 (1997). - PubMed
-
- Iranzo, A. et al. Detection of α-synuclein in CSF by RT-QuIC in patients with isolated rapid-eye-movement sleep behaviour disorder: a longitudinal observational study. Lancet Neurol.20, 203–212 (2021). - PubMed
MeSH terms
Substances
Grants and funding
- 21dm0207070/Japan Agency for Medical Research and Development (AMED)
- 21wm0425015/Japan Agency for Medical Research and Development (AMED)
- 21H04820/MEXT | Japan Society for the Promotion of Science (JSPS)
- 19K16928/MEXT | Japan Society for the Promotion of Science (JSPS)
- 21K07424/MEXT | Japan Society for the Promotion of Science (JSPS)
