

Chen's penetrating-suture technique for pancreaticojejunostomy following pancreaticoduodenectomy
- PMID: 37248522
- PMCID: PMC10228121
- DOI: 10.1186/s12893-023-02054-y
Chen's penetrating-suture technique for pancreaticojejunostomy following pancreaticoduodenectomy
Abstract
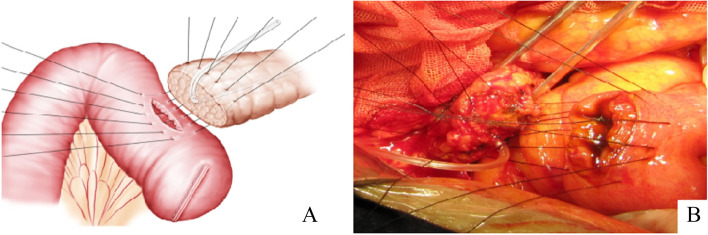
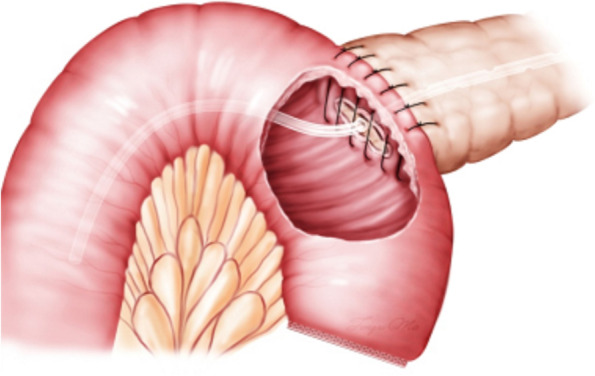
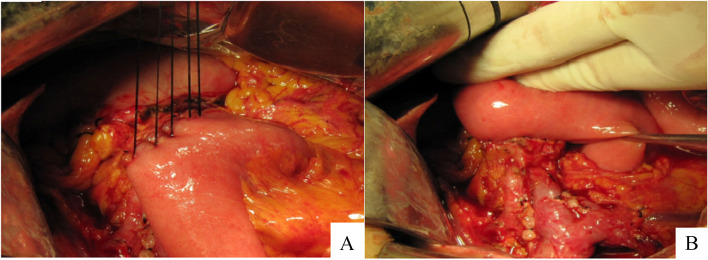
Background: Postoperative pancreatic fistula (POPF) is the most serious complication and the main reason for morbidity and mortality after pancreaticoduodenectomy (PD). Currently, there exists no flawless pancreaticojejunal anastomosis approach. We presents a new approach called Chen's penetrating-suture technique for pancreaticojejunostomy (PPJ), which involves end-to-side pancreaticojejunostomy by suture penetrating the full-thickness of the pancreas and jejunum, and evaluates its safety and efficacy.
Methods: To assess this new approach, between May 2006 and July 2018, 193 consecutive patients who accepted the new Chen's Penetrating-Suture technique after a PD were enrolled in this study. Postoperative morbidity and mortality were evaluated.
Results: All cases recovered well after PD. The median operative time was 256 (range 208-352) min, with a median time of 12 (range 8-25) min for performing pancreaticojejunostomy. Postoperative morbidity was 19.7% (38/193) and mortality was zero. The POPF rate was 4.7% (9/193) for Grade A, 1.0% (2/193) for Grade B, and no Grade C cases and one urinary tract infection.
Conclusion: PPJ is a simple, safe, and reliable technique with ideal postoperative clinical results.
Keywords: Chen’s Penetrating-Suture technique; Pancreaticoduodenectomy; Postoperative pancreatic fistula.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
