

Determinants of door-in-door-out time in patients with ischaemic stroke transferred for endovascular thrombectomy
- PMID: 37248995
- PMCID: PMC10472962
- DOI: 10.1177/23969873231177768
Determinants of door-in-door-out time in patients with ischaemic stroke transferred for endovascular thrombectomy
Abstract
Background: Long door-in-door-out (DIDO) times are an important cause of treatment delay in patients transferred for endovascular thrombectomy (EVT) from primary stroke centres (PSC) to an intervention centre. Insight in causes of prolonged DIDO times may facilitate process improvement interventions. We aimed to quantify different components of DIDO time and to identify determinants of DIDO time.
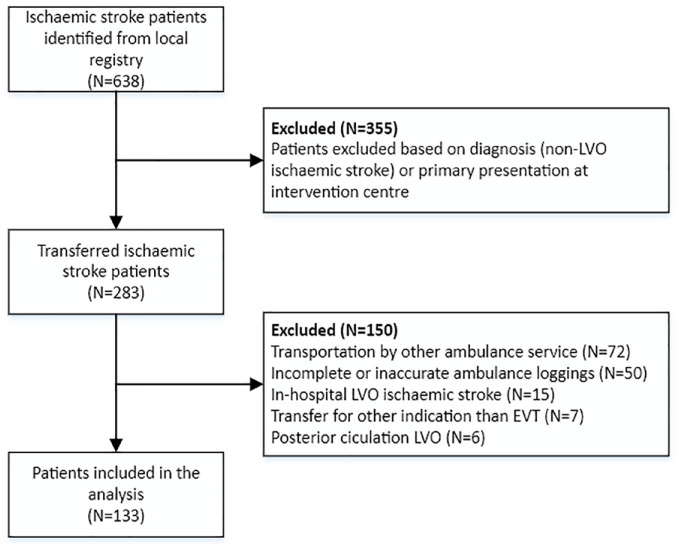
Methods: We performed a retrospective cohort study in a Dutch ambulance region consisting of six PSCs and one intervention centre. We included consecutive adult patients with anterior circulation large vessel occlusion, transferred from a PSC for EVT between October 1, 2019 and November 31, 2020. We subdivided DIDO into several time components and quantified contribution of these components to DIDO time. We used univariable and multivariable linear regression models to explore associations between potential determinants and DIDO time.
Results: We included 133 patients. Median (IQR) DIDO time was 66 (52-83) min. The longest component was CTA-to-ambulance notification time with a median (IQR) of 24 (16-37) min. DIDO time increased with age (6 min per 10 years, 95% CI: 2-9), onset-to-door time outside 6 h (20 min, 95% CI: 5-35), M2-segment occlusion (15 min, 95% CI: 4-26) and right-sided ischaemia (12 min, 95% CI: 2-21).
Conclusions: The CTA-to-ambulance notification time is the largest contributor to DIDO time. Higher age, onset-to-door time longer than 6 h, M2-segment occlusion and right-sided occlusions are independently associated with a longer DIDO time. Future interventions that aim to decrease DIDO time should take these findings into account.
Keywords: Ischaemic stroke; door-in-door-out time; endovascular thrombectomy; hospital workflow.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Diederik Dippel reports funding from the Dutch Heart Foundation, Brain Foundation Netherlands, The Netherlands Organisation for Health Research and Development, Health Holland Top Sector Life Sciences & Health, and unrestricted grants from Penumbra Inc., Stryker, Stryker European Operations BV, Medtronic, Thrombolytic Science, LLC and Cerenovus for research, all paid to institution. Bob Roozenbeek reports funding from the Dutch Heart Foundation and The Netherlands Organisation for Health Research and Development, all paid to institution. All other authors declare no conflict of interest.
References
-
- Saver JL, Goyal M, van der Lugt A, et al.. Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: a meta-analysis. JAMA 2016; 316: 1279–1288. - PubMed
-
- Hacke W, Kaste M, Bluhmki E, et al.. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008; 359: 1317–1329. - PubMed
-
- Ma H, Campbell BCV, Parsons MW, et al.. Thrombolysis guided by perfusion imaging up to 9 hours after onset of stroke. N Engl J Med 2019; 380: 1795–1803. - PubMed
-
- Goyal M, Menon BK, van Zwam WH, et al.. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet 2016; 387: 1723–1731. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
