

Immune checkpoint inhibitors efficacy across solid cancers and the utility of PD-L1 as a biomarker of response: a systematic review and meta-analysis
- PMID: 37250628
- PMCID: PMC10219231
- DOI: 10.3389/fmed.2023.1192762
Immune checkpoint inhibitors efficacy across solid cancers and the utility of PD-L1 as a biomarker of response: a systematic review and meta-analysis
Abstract
Background: Immune checkpoint inhibitors (ICPI) are a tumor agnostic treatment. However, trials of their use have been site specific. Here we summarize the trial data and explore the utility of programmed death-ligand 1 (PD-L1) expression as a biomarker to direct their pan-cancer use.
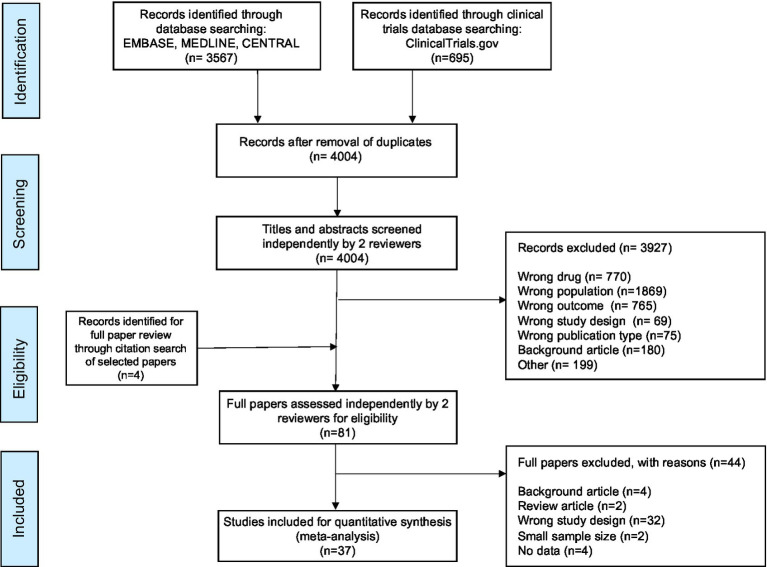
Method: A systematic review of literature, following PRISMA guidelines, was performed. Medline, Embase, Cochrane CENTRAL, NHS Health and Technology, and Web of Science were searched from their conception to June 2022 limited to the English language. The search terms and method were devised by a specialist medical librarian. Studies were limited to adults with solid cancers (excluding melanomas) treated with ICPIs. Only phase III randomized control trials (RCT) were included. The primary outcome was overall survival and secondary outcomes were progression free survival, PD-L1 expression, quality of life outcomes and adverse event data. Where present in eligible clinical trials, hazard ratios (HR), risk ratios (RR), standard error (SE) and 95% confidence intervals (CI) were extracted or calculated. Heterogeneity across studies was described with the use of an I2 score (Low: 25, 50%: moderate, 75% low heterogeneity). HR pools inverse variance methods were adopted by Random Effects (RE). Means were standardized across any heterogenous scale limits.
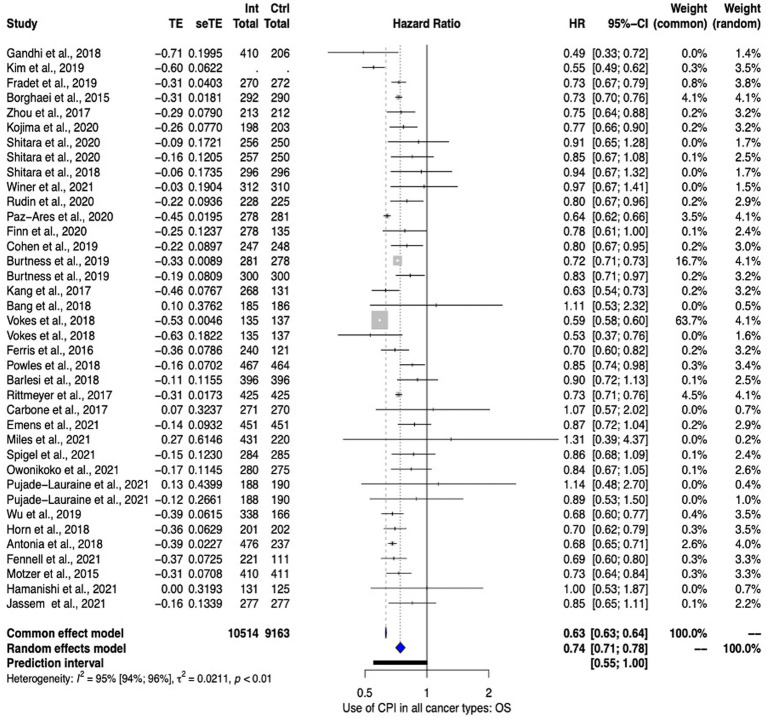
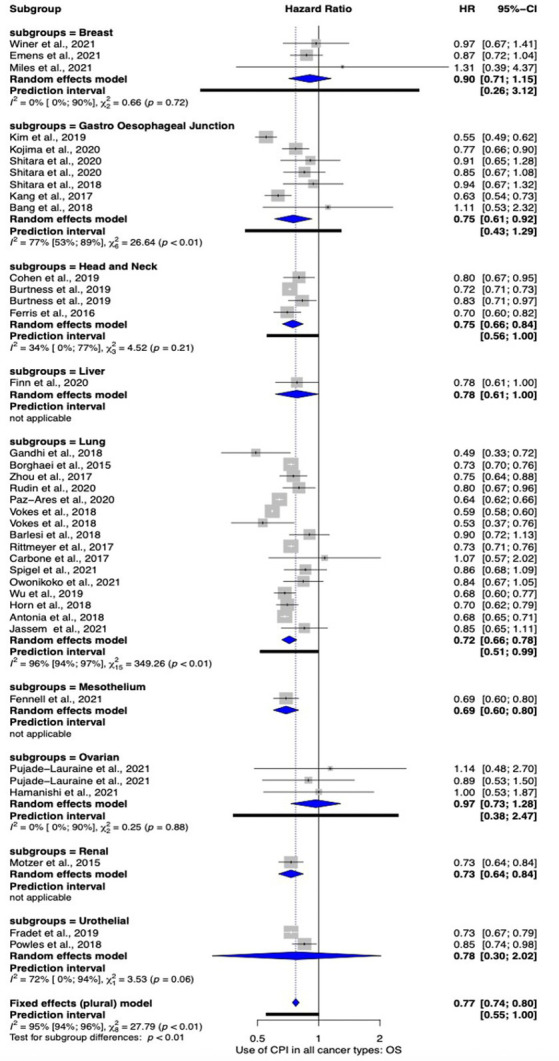
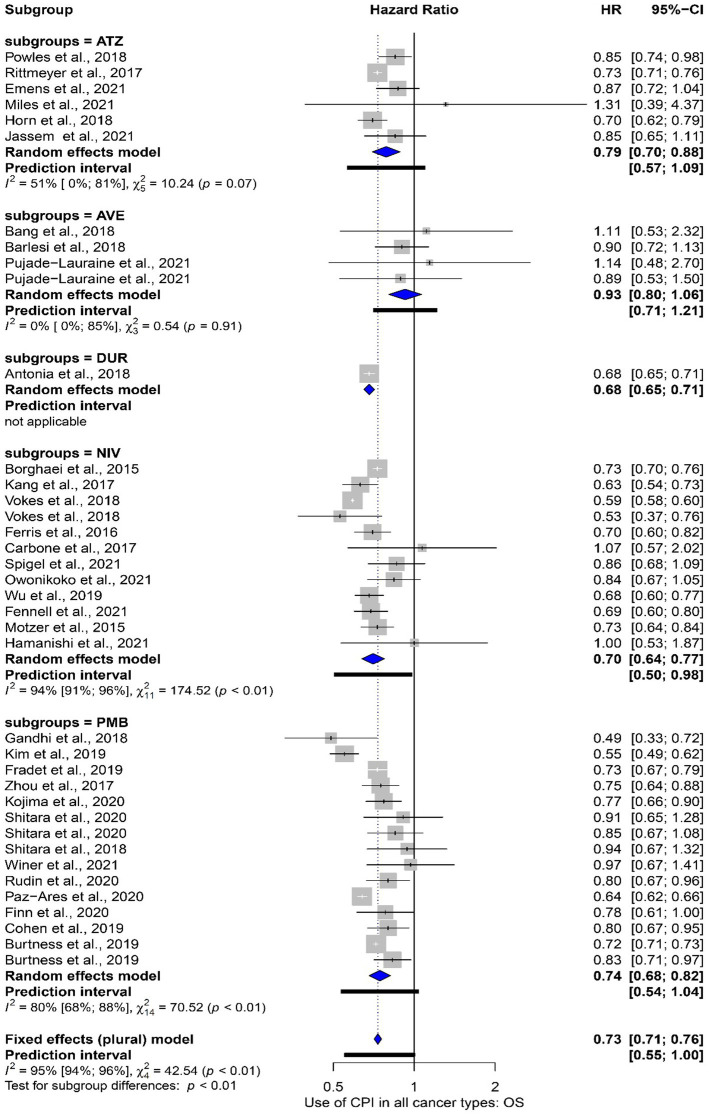
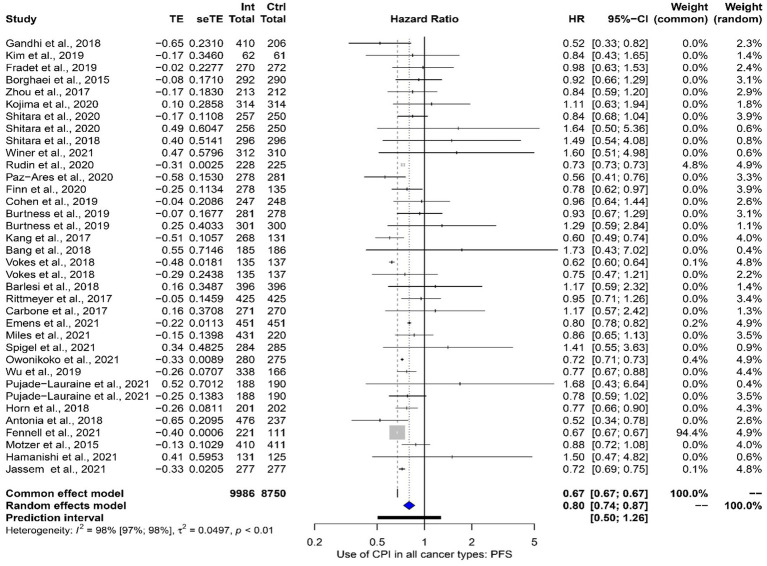
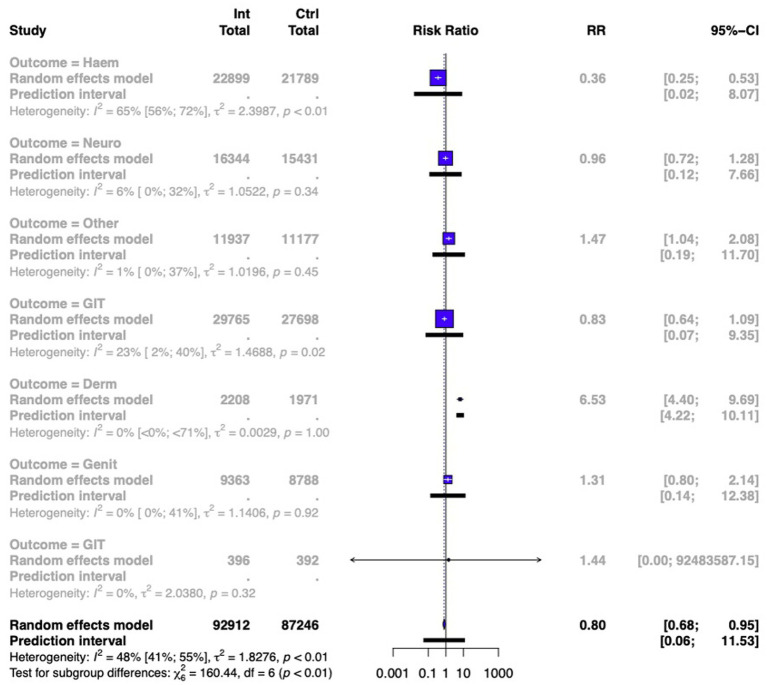
Results: In total 46,510 participants were included in the meta-analysis. Overall, meta-analysis favored the use of ICPIs with an overall survival (OS) HR of 0.74 (95% CI 0.71 to 0.78). Lung cancers showed the most benefit in OS [HR 0.72 (95% 0.66-0.78)] followed by head and neck cancers [HR 0.75 (95% CI 0.66-0.84)] and gastroesophageal junction cancers [HR 0.75 (95% CI 0.61-0.92)]. ICPIs seem to be efficacious at both primary presentation and recurrence [OS HR 0.73 (95% CI 0.68-0.77)] vs. [OS HR 0.79 (95% CI 0.72 to 0.87)] respectively. Interestingly, subgroup analysis comparing studies in which most cancers demonstrated PD-L1 expression vs. those studies in which a minority of cancer demonstrated PD-L1 expression reported similar effect of ICPI use on OS; oddly the data favored ICPI use in studies with a minority of PD-L1 expression. Specifically, studies with minority PD-L1 expression had an HR 0.73 (95% CI 0.68-0.78) vs. studies with majority PD-L1 expression HR 0.76 (95% CI 0.70-0.84). This was maintained even when studies exploring the same cancer site were directly compared. Subgroup analysis was performed comparing the impact on OS subdivided by the specific ICPI used. Where meta-analysis was performed, Nivolumab led to the greatest impact [HR 0.70 (95% CI 0.64-0.77)] with Avelumab failing to reach significance [HR 0.93 (95% CI 0.80-1.06)]. However, overall heterogenicity was high (I2 = 95%). Finally, the use of ICPIs led to an improved side effect profile when compared with standard chemotherapy [RR 0.85 (95% CI 0.73-0.98)].
Conclusion: ICPIs improve survival outcomes in all cancer types. These effects are seen in the primary, recurrent, chemotherapy sensitive, chemotherapy resistant disease. These data support their use as a tumor agnostic therapy. Furthermore, they are well tolerated. However, PD-L1 as a biomarker for the targeting of ICPI use seems problematic. Other biomarkers such as mismatch repair or tumor mutational burden should be explored in randomized trials. In addition, there are still limited trials looking at ICPI use outside of lung cancer.
Keywords: PDL1; checkpoint immune blockade antibodies; immunotherapy; mismatch repair; oncology; pan-cancer therapy.
Copyright © 2023 Fitzsimmons, Singh, Walker, Newton, Evans, Crosbie and Ryan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- GBD 2017 Causes of Death Collaborators . Global, regional, And national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1736–88. doi: 10.1016/s0140-6736(18)32203-7, PMID: - DOI - PMC - PubMed
-
- Gerber DE. Targeted therapies: a new generation of cancer treatments. Am Fam Physician. (2008) 77:311–9. Available at: https://pubmed.ncbi.nlm.nih.gov/18297955/ PMID: - PubMed
LinkOut - more resources
Full Text Sources
Research Materials