

Long-term use of somatostatin analogs for chronic gastrointestinal bleeding in hereditary hemorrhagic telangiectasia
- PMID: 37250655
- PMCID: PMC10213420
- DOI: 10.3389/fmed.2023.1146080
Long-term use of somatostatin analogs for chronic gastrointestinal bleeding in hereditary hemorrhagic telangiectasia
Abstract
Background: Chronic bleeding due to gastrointestinal (GI) involvement in patients with hemorrhagic hereditary telangiectasia (HHT) can provoke severe anemia with high red blood cells (RBC) transfusion requirements. However, the evidence about how to deal with these patients is scarce. We aimed to assess the long-term efficacy and safety of somatostatin analogs (SA) for anemia management in HHT patients with GI involvement.
Methods: This is a prospective observational study including patients with HHT and GI involvement attended at a referral center. SA were considered for those patients with chronic anemia. Anemia-related variables were compared in patients receiving SA before and during treatment. Patients receiving SA were divided into responders (patients with minimal hemoglobin levels improvement >10 g/L and maintaining hemoglobin levels ≥80 g/L during treatment), and non-responders. Adverse effects during follow-up were collected.
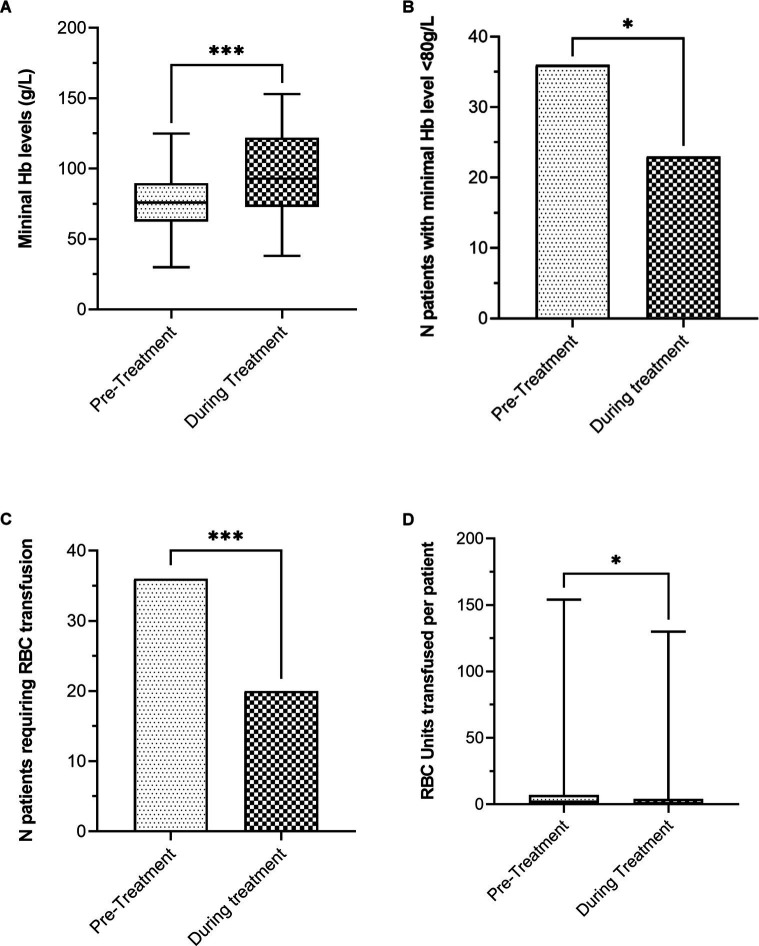
Results: Among 119 HHT patients with GI involvement, 67 (56.3%) received SA. These patients showed lower minimal hemoglobin levels (73 [60-87] vs. 99 [70.2-122.5], p < 0.001), and more RBC transfusion requirements (61.2% vs. 38.5%, p = 0.014) than patients without SA therapy. Median treatment period was 20.9 ± 15.2 months. During treatment, there was a statistically significant improvement in minimum hemoglobin levels (94.7 ± 29.8 g/L vs. 74.7 ± 19.7, p < 0.001) and a reduction of patients with minimal hemoglobin levels <80 g/L (39 vs. 61%, p = 0.007) and RBC transfusions requirement (33.9% vs. 59.3%, p < 0.001). Sixteen (23.9%) patients showed mild adverse effects, mostly diarrhea or abdominal pain, leading to treatment discontinuation in 12 (17.9%) patients. Fifty-nine patients were eligible for efficacy assessment and 32 (54.2%) of them were considered responders. Age was associated with non-responder patients, OR 95% CI; 1.070 (1.014-1.130), p = 0.015.
Conclusion: SA can be considered a long-term effective and safe option for anemia management in HHT patients with GI bleeding. Older age is associated with poorer response.
Keywords: anemia; gastrointestinal bleeding; hereditary hemorrhagic telangectasia; rare diseases; somatostatin analogs.
Copyright © 2023 Torres-Iglesias, Mora-Luján, Iriarte, Cerdà, Alba, Sánchez-Corral, Berrozpe, Cruellas, Gamundí, Ribas, Castellote and Riera-Mestre.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Pazopanib for severe bleeding and transfusion-dependent anemia in hereditary hemorrhagic telangiectasia.Angiogenesis. 2022 Feb;25(1):87-97. doi: 10.1007/s10456-021-09807-4. Epub 2021 Jul 22. Angiogenesis. 2022. PMID: 34292451 Free PMC article.
-
Gastrointestinal Bleeding in Patients with Hereditary Hemorrhagic Telangiectasia: Risk Factors and Endoscopic Findings.J Clin Med. 2019 Dec 28;9(1):82. doi: 10.3390/jcm9010082. J Clin Med. 2019. PMID: 31905627 Free PMC article.
-
Intravenous Bevacizumab for Refractory Hereditary Hemorrhagic Telangiectasia-Related Epistaxis and Gastrointestinal Bleeding.Mayo Clin Proc. 2018 Feb;93(2):155-166. doi: 10.1016/j.mayocp.2017.11.013. Epub 2018 Jan 24. Mayo Clin Proc. 2018. PMID: 29395350
-
Effectiveness and predictors of response to somatostatin analogues in patients with gastrointestinal angiodysplasias: a systematic review and individual patient data meta-analysis.Lancet Gastroenterol Hepatol. 2021 Nov;6(11):922-932. doi: 10.1016/S2468-1253(21)00262-4. Epub 2021 Sep 9. Lancet Gastroenterol Hepatol. 2021. PMID: 34508668
-
Systemic Antiangiogenic Therapies for Bleeding in Hereditary Hemorrhagic Telangiectasia: A Practical, Evidence-Based Guide for Clinicians.Semin Thromb Hemost. 2022 Jul;48(5):514-528. doi: 10.1055/s-0042-1743467. Epub 2022 Feb 28. Semin Thromb Hemost. 2022. PMID: 35226946 Review.
Cited by
-
Aflibercept for Gastrointestinal Bleeding in Hereditary Hemorrhagic Telangiectasia: A Case Report.Medicina (Kaunas). 2023 Aug 24;59(9):1533. doi: 10.3390/medicina59091533. Medicina (Kaunas). 2023. PMID: 37763652 Free PMC article.
-
How I treat bleeding in hereditary hemorrhagic telangiectasia.Blood. 2024 Aug 29;144(9):940-954. doi: 10.1182/blood.2023021765. Blood. 2024. PMID: 38864625 Free PMC article.
References
-
- Orphanet: an online rare disease and orphan drug data base . © INSERM (1999). Available at: http://www.orpha.net (Accessed June 13, 2022).
-
- Donaldson JW, McKeever TM, Hall IP, Hubbard RB, Fogarty AW. The UK prevalence of hereditary haemorrhagic telangiectasia and its association with sex, socioeconomic status and region of residence: a population-based study. Thorax. (2014) 69:161–7. doi: 10.1136/thoraxjnl-2013-203720, PMID: - DOI - PubMed
-
- Faughnan ME, Palda VA, Garcia-Tsao G, Geisthoff UW, McDonald J, Proctor DD, et al. . HHT Foundation International - guidelines working group. International guidelines for the diagnosis and management of hereditary haemorrhagic telangiectasia. J Med Genet. (2011) 48:73–87. doi: 10.1136/jmg.2009.069013, PMID: - DOI - PubMed