

Identifying and Mitigating Disparities in Central Line-Associated Bloodstream Infections in Minoritized Racial, Ethnic, and Language Groups
- PMID: 37252746
- PMCID: PMC10230370
- DOI: 10.1001/jamapediatrics.2023.1379
Identifying and Mitigating Disparities in Central Line-Associated Bloodstream Infections in Minoritized Racial, Ethnic, and Language Groups
Abstract
Importance: Although inequitable care due to racism and bias is well documented in health care, the impact on health care-associated infections is less understood.
Objective: To determine whether disparities in first central catheter-associated bloodstream infection (CLABSI) rates existed for pediatric patients of minoritized racial, ethnic, and language groups and to evaluate the outcomes associated with quality improvement initiatives for addressing these disparities.
Design, setting, and participants: This cohort study retrospectively examined outcomes of 8269 hospitalized patients with central catheters from October 1, 2012, to September 30, 2019, at a freestanding quaternary care children's hospital. Subsequent quality improvement interventions and follow-up were studied, excluding catheter days occurring after the outcome and episodes with catheters of indeterminate age through September 2022.
Exposures: Patient self-reported (or parent/guardian-reported) race, ethnicity, and language for care as collected for hospital demographic purposes.
Main outcomes and measures: Central catheter-associated bloodstream infection events identified by infection prevention surveillance according to National Healthcare Safety Network criteria were reported as events per 1000 central catheter days. Cox proportional hazards regression was used to analyze patient and central catheter characteristics, and interrupted time series was used to analyze quality improvement outcomes.
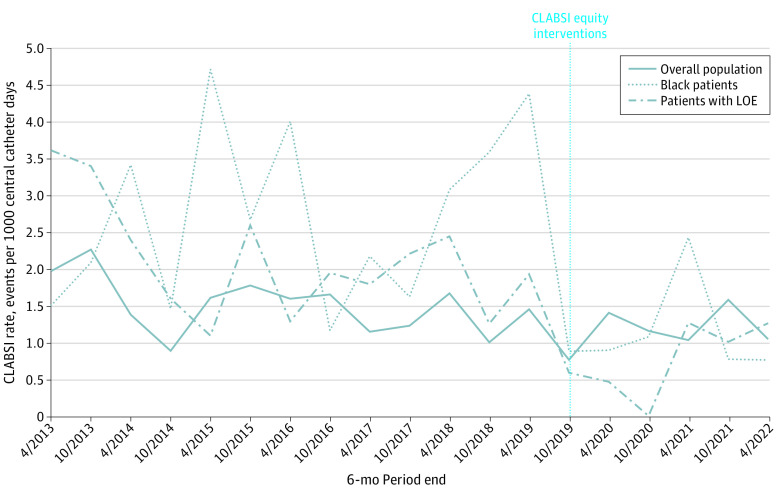
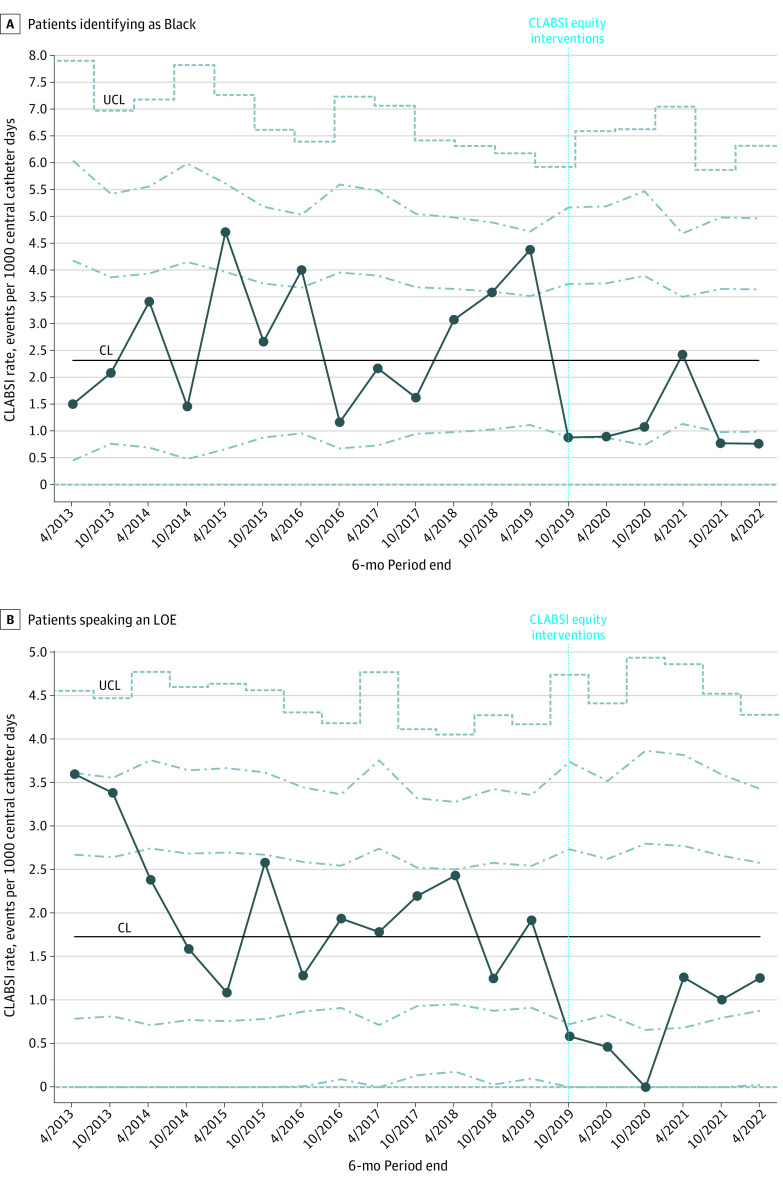
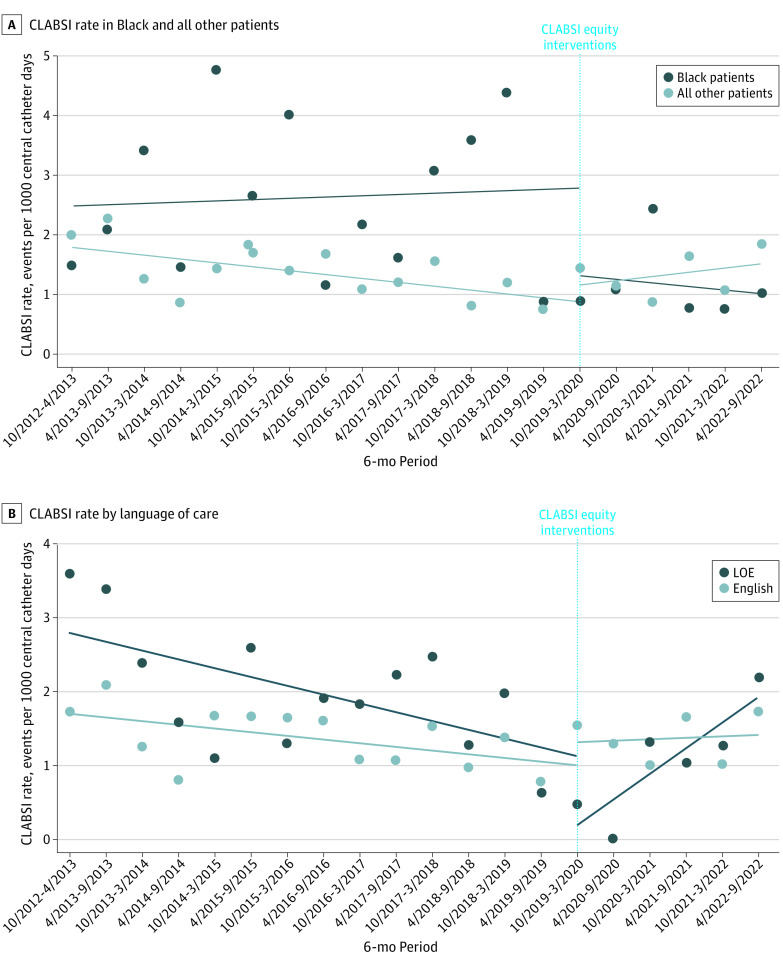
Results: Unadjusted infection rates were higher for Black patients (2.8 per 1000 central catheter days) and patients who spoke a language other than English (LOE; 2.1 per 1000 central catheter days) compared with the overall population (1.5 per 1000 central catheter days). Proportional hazard regression included 225 674 catheter days with 316 infections and represented 8269 patients. A total of 282 patients (3.4%) experienced a CLABSI (mean [IQR] age, 1.34 [0.07-8.83] years; female, 122 [43.3%]; male, 160 [56.7%]; English-speaking, 236 [83.7%]; LOE, 46 [16.3%]; American Indian or Alaska Native, 3 [1.1%]; Asian, 14 [5.0%]; Black, 26 [9.2%]; Hispanic, 61 [21.6%]; Native Hawaiian or Other Pacific Islander, 4 [1.4%]; White, 139 [49.3%]; ≥2 races, 14 [5.0%]; unknown race and ethnicity or refused to answer, 15 [5.3%]). In the adjusted model, a higher hazard ratio (HR) was observed for Black patients (adjusted HR, 1.8; 95% CI, 1.2-2.6; P = .002) and patients who spoke an LOE (adjusted HR, 1.6; 95% CI, 1.1-2.3; P = .01). Following quality improvement interventions, infection rates in both subgroups showed statistically significant level changes (Black patients: -1.77; 95% CI, -3.39 to -0.15; patients speaking an LOE: -1.25; 95% CI, -2.23 to -0.27).
Conclusions and relevance: The study's findings show disparities in CLABSI rates for Black patients and patients who speak an LOE that persisted after adjusting for known risk factors, suggesting that systemic racism and bias may play a role in inequitable hospital care for hospital-acquired infections. Stratifying outcomes to assess for disparities prior to quality improvement efforts may inform targeted interventions to improve equity.
Conflict of interest statement
Figures
Similar articles
-
Racial and Ethnic Disparities in All-Cause and Cause-Specific Mortality Among US Youth.JAMA. 2024 May 28;331(20):1732-1740. doi: 10.1001/jama.2024.3908. JAMA. 2024. PMID: 38703403 Free PMC article.
-
Racial and ethnic disparities in healthcare-associated infections in the United States, 2009-2011.Infect Control Hosp Epidemiol. 2014 Oct;35 Suppl 3:S10-6. doi: 10.1086/677827. Infect Control Hosp Epidemiol. 2014. PMID: 25222888
-
Racial/Ethnic Disparities in the Performance of Prediction Models for Death by Suicide After Mental Health Visits.JAMA Psychiatry. 2021 Jul 1;78(7):726-734. doi: 10.1001/jamapsychiatry.2021.0493. JAMA Psychiatry. 2021. PMID: 33909019 Free PMC article.
-
Race and Ethnicity Representation in Phase 2/3 Oncology Clinical Trial Publications: A Systematic Review.JAMA Health Forum. 2024 Jun 7;5(6):e241388. doi: 10.1001/jamahealthforum.2024.1388. JAMA Health Forum. 2024. PMID: 38848090 Free PMC article.
-
Assessment of the Inclusion of Racial/Ethnic Minority, Female, and Older Individuals in Vaccine Clinical Trials.JAMA Netw Open. 2021 Feb 1;4(2):e2037640. doi: 10.1001/jamanetworkopen.2020.37640. JAMA Netw Open. 2021. PMID: 33606033 Free PMC article. Review.
Cited by
-
Ascertaining provider-level implicit bias in electronic health records with rules-based natural language processing: A pilot study in the case of prostate cancer.PLoS One. 2024 Dec 30;19(12):e0314989. doi: 10.1371/journal.pone.0314989. eCollection 2024. PLoS One. 2024. PMID: 39775249 Free PMC article.
-
Prioritizing Equity in Antimicrobial Stewardship Efforts (EASE): a framework for infectious diseases clinicians.Antimicrob Steward Healthc Epidemiol. 2024 May 3;4(1):e74. doi: 10.1017/ash.2024.69. eCollection 2024. Antimicrob Steward Healthc Epidemiol. 2024. PMID: 38721493 Free PMC article. Review.
-
Making lemonade out of lemons: an approach to combining variable race and ethnicity data from hospitals for quality and safety efforts.BMJ Qual Saf. 2024 Jan 19;33(2):74-77. doi: 10.1136/bmjqs-2023-016438. BMJ Qual Saf. 2024. PMID: 37714699 Free PMC article. No abstract available.
-
Access and Inequities: Differential Effects of Digital Access by Race, Ethnicity, and Language.J Pediatr. 2024 Feb;265:113825. doi: 10.1016/j.jpeds.2023.113825. Epub 2023 Nov 17. J Pediatr. 2024. PMID: 37977330 Free PMC article. No abstract available.
-
National partnerships address critical needs in infection prevention and control.Antimicrob Steward Healthc Epidemiol. 2024 Dec 2;4(1):e213. doi: 10.1017/ash.2024.447. eCollection 2024. Antimicrob Steward Healthc Epidemiol. 2024. PMID: 39654591 Free PMC article.
References
-
- Akinboyo IC, Young RR, Smith MJ, Lewis SS, Smith BA, Anderson DJ. Burden of healthcare-associated infections among hospitalized children within community hospitals participating in an infection control network. Infect Control Hosp Epidemiol. 2022;43(4):510-512. doi:10.1017/ice.2021.67 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
