

Three-month outcomes of faricimab loading therapy for wet age-related macular degeneration in Japan
- PMID: 37253802
- PMCID: PMC10229564
- DOI: 10.1038/s41598-023-35759-4
Three-month outcomes of faricimab loading therapy for wet age-related macular degeneration in Japan
Abstract
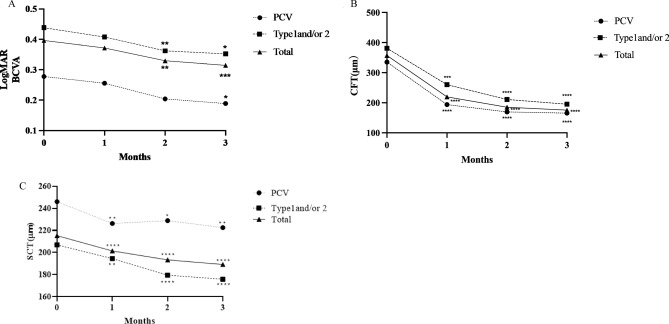
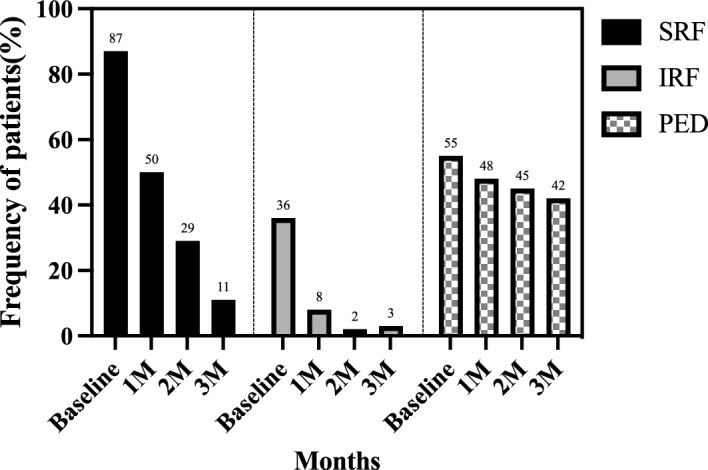
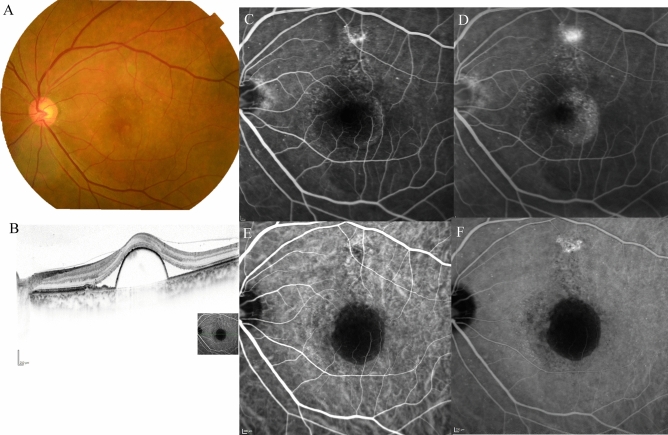
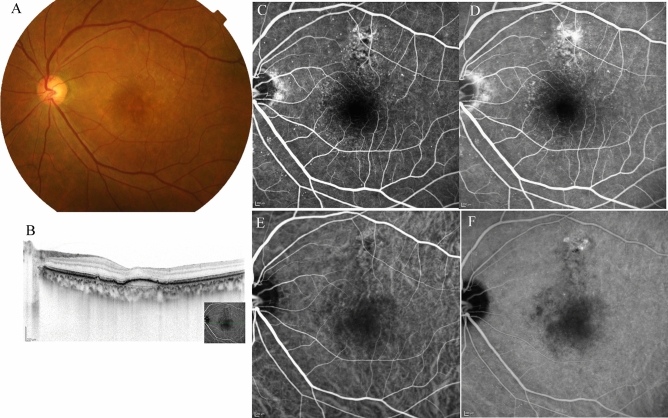
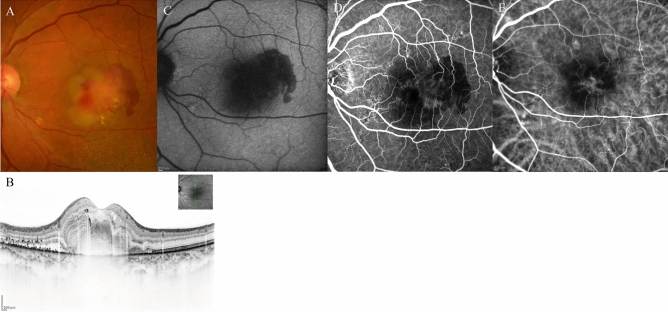
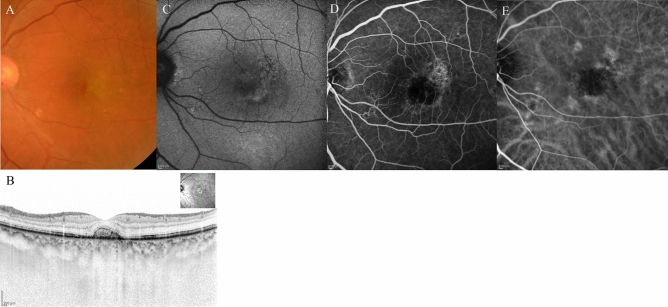
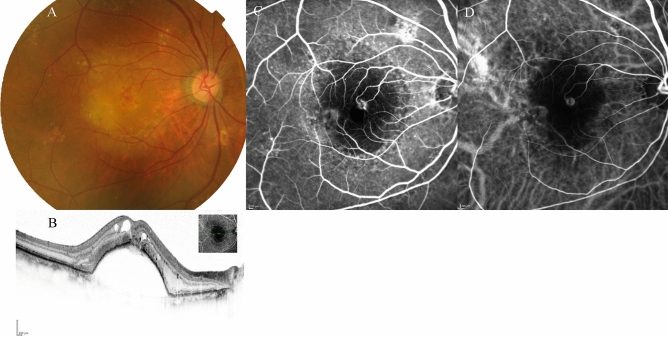
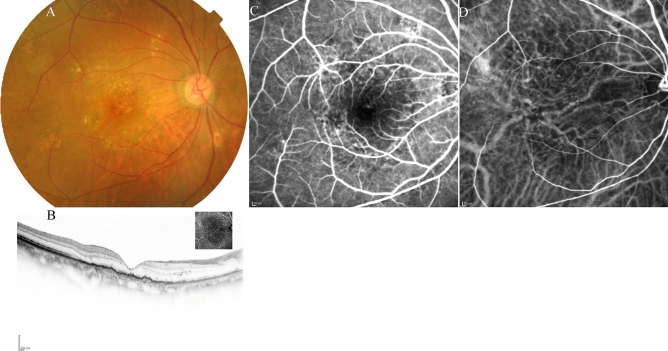
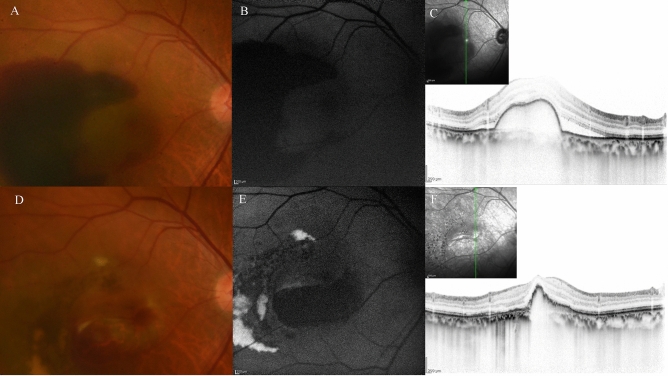
This multicenter study aimed to assess the short-term effectiveness and safety of faricimab in treatment-naïve patients with wet age-related macular degeneration (wAMD) in Japan. We retrospectively reviewed 63 eyes of 61 patients with wAMD, including types 1, 2, and 3 macular neovascularization as well as polypoidal choroidal vasculopathy (PCV). Patients received three consecutive monthly intravitreal injections of faricimab as loading therapy. Over these 3 months, visual acuity improved gradually compared to baseline. Moreover, the central foveal thickness decreased significantly at 1, 2, and 3 months compared to baseline (p < 0.0001). At 3 months after initiation of faricimab therapy, a dry macula (defined as absence of intraretinal or subretinal fluid) was achieved in 82% of the eyes. Complete regression of polypoidal lesions was observed in 52% of eyes with PCV. Subfoveal choroidal thickness also decreased significantly at 1, 2, and 3 months compared to baseline (p < 0.0001). Although retinal pigment epithelium tears developed in two eyes, there were no other ocular or systemic complications observed during the 3 months of loading therapy. In conclusion, loading therapy using faricimab resulted in improved visual acuity and retinal morphology in Japanese patients with wAMD without particular safety issues.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Klaver CC, et al. Incidence and progression rates of age-related maculopathy: The Rotterdam Study. Invest Ophthalmol. Vis. Sci. 2001;42:2237–2241. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
