

ILC2 regulates hyperoxia-induced lung injury via an enhanced Th17 cell response in the BPD mouse model
- PMID: 37254088
- PMCID: PMC10230686
- DOI: 10.1186/s12890-023-02474-9
ILC2 regulates hyperoxia-induced lung injury via an enhanced Th17 cell response in the BPD mouse model
Abstract
Backgroud: Recent research has focused on the role of immune cells and immune responses in the pathogenesis of bronchopulmonary dysplasia (BPD), but the exact mechanisms have not yet been elucidated. Previously, the key roles of type 2 innate lymphoid cells (ILC2) in the lung immune network of BPD were explored. Here, we investigated the role Th17 cell response in hyperoxia-induced lung injury of BPD, as well as the relationship between ILC2 and Th17 cell response.
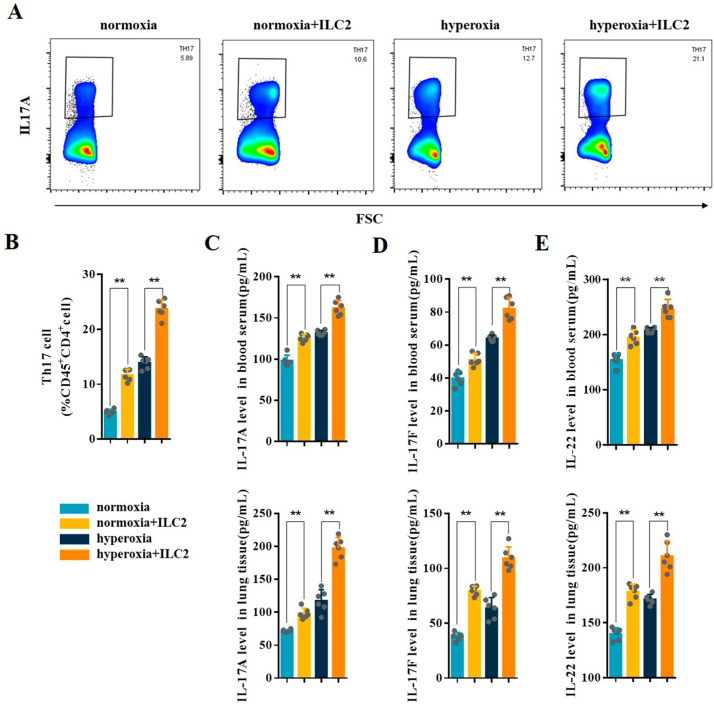
Methods: A hyperoxia-induced BPD mouse model was constructed and the pathologic changes of lung tissues were evaluated by Hematoxylin-Eosin staining. Flow cytometry analysis was conducted to determine the levels of Th17 cell, ILC2 and IL-6+ILC2. The expression levels of IL-6, IL-17 A, IL-17 F, and IL-22 in the blood serum and lung tissues of BPD mice were measured by ELISA. To further confirm the relationship between ILC2 and Th17 cell differentiation, ILC2 depletion was performed in BPD mice. Furthermore, we used immunomagnetic beads to enrich ILC2 and then flow-sorted mouse lung CD45+Lin-CD90.2+Sca-1+ILC2. The sorted ILC2s were injected into BPD mice via tail vein. Following ILC2 adoptive transfusion, the changes of Th17 cell response and lung injury were detected in BPD mice.
Results: The expression levels of Th17 cells and Th17 cell-related cytokines, including IL-17 A, IL-17 F, and IL-22, were significantly increased in BPD mice. Concurrently, there was a significant increase in the amount of ILC2 and IL-6+ILC2 during hyperoxia-induced lung injury, which was consistent with the trend for Th17 cell response. Compared to the control BPD group, ILC2 depletion was found to partially abolish the Th17 cell response and had protective effects against lung injury after hyperoxia. Furthermore, the adoptive transfer of ILC2 enhanced the Th17 cell response and aggravated lung injury in BPD mice.
Conclusions: This study found that ILC2 regulates hyperoxia-induced lung injury by targeting the Th17 cell response in BPD, which shows a novel strategy for BPD immunotherapy.
Keywords: Bronchopulmonary dysplasia; Lung injury; Th17 cell response; Type 2 innate lymphoid cells.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures








References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
