

Integration of Multi-omic Data in a Molecular Tumor Board Reveals EGFR-Associated ALK-Inhibitor Resistance in a Patient With Inflammatory Myofibroblastic Cancer
- PMID: 37255276
- PMCID: PMC10400139
- DOI: 10.1093/oncolo/oyad129
Integration of Multi-omic Data in a Molecular Tumor Board Reveals EGFR-Associated ALK-Inhibitor Resistance in a Patient With Inflammatory Myofibroblastic Cancer
Abstract
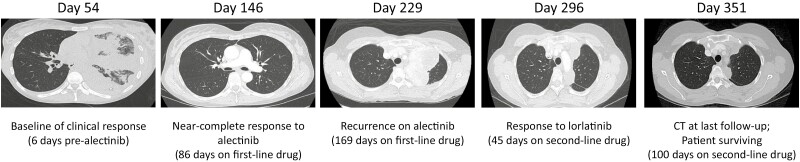
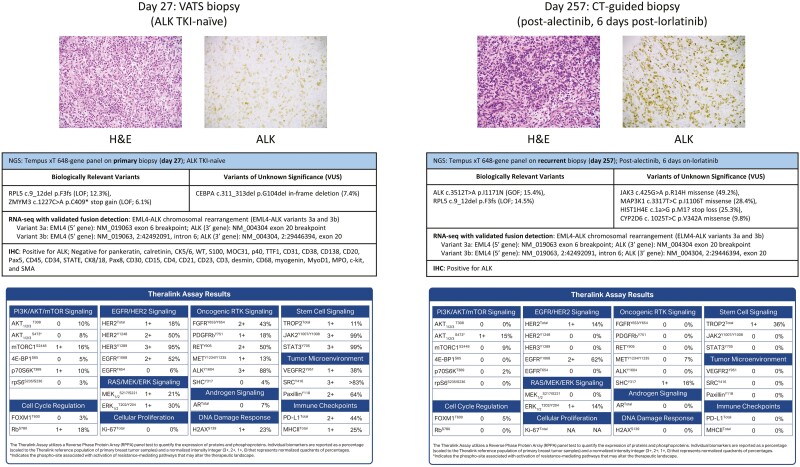
Inflammatory myofibroblastic tumors (IMTs) are intermediate-grade mesenchymal neoplasms commonly characterized by chromosomal rearrangements causing constitutive activation of anaplastic lymphoma kinase (ALK) and/or ALK mutations causing reduced sensitivity to ALK tyrosine kinase inhibitors (TKI). We present a patient with an IMT who initially responded to first-line alectinib, but who later suffered disease relapse and presently survives with moderate residual disease after receiving second-line lorlatinib. Biopsy specimens were analyzed using next generation sequencing (DNA-seq and RNA-seq) and reverse phase protein microarray (RPPA) as part of an institutional Molecular Tumor Board (MTB) study. An EML4-ALK rearrangement and EGFR activation (pEGFRY1068) were present in both the primary and recurrent tumors, while a secondary ALK I1171N mutation was exclusive to the latter. EGFR signaling in the background of a secondary ALK mutation is correlated with reduced ALK TKI sensitivity in vitro, implicating an important mechanism of drug resistance development in this patient. The RPPA results also critically demonstrate that ALK signaling (ALKY1604) was not activated in the recurrent tumor, thereby indicating that standard-of-care use of third- or fourth-line ALK TKI would not likely be efficacious or durable. These results underscore the importance of real-time clinical integration of functional protein drug target activation data with NGS in the MTB setting for improving selection of patient-tailored therapy.
Keywords: DNA sequencing; inflammatory myofibroblastic tumor; proteogenomics; proteomics; reverse phase protein microarray.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
Emanuel F. Petricoin reported consulting and advisory role with Theralink Technologies, Inc., Perthera, Inc., and Ceres Nanosciences, Inc., and research funding from Deciphera Therapeutics, Springwork Therapeutics, Genentech, AbbVie, and Peytant Solutions. Thomas P. Conrads reported consulting or advisory role with ThermoFisher Scientific, Inc., and research funding from AbbVie. Timothy L. Cannon is a paid member of the molecular tumor board for Intermountain Health. The other authors indicated no financial relationships.
Figures

Similar articles
-
Treatment of Brain Metastases of Non-Small Cell Lung Carcinoma.Int J Mol Sci. 2021 Jan 8;22(2):593. doi: 10.3390/ijms22020593. Int J Mol Sci. 2021. PMID: 33435596 Free PMC article. Review.
-
Detection of an EML4-ALK fusion mutation secondary to epidermal growth factor receptor-tyrosine kinase inhibitor (EGFR-TKI) therapy for lung cancer: a case report.Ann Palliat Med. 2022 Jul;11(7):2503-2509. doi: 10.21037/apm-22-744. Ann Palliat Med. 2022. PMID: 35927783
-
A case report: Pharmacology and resistance patterns of three generations of ALK inhibitors in metastatic inflammatory myofibroblastic sarcoma.J Oncol Pharm Pract. 2019 Jul;25(5):1226-1230. doi: 10.1177/1078155218781944. Epub 2018 Jun 20. J Oncol Pharm Pract. 2019. PMID: 29925295
-
An Inflammatory Myofibroblastic Tumor With a Novel ALKV1180L Mutation Leading to Acquired Resistance to Tyrosine Kinase Inhibitors.Genes Chromosomes Cancer. 2024 Nov;63(11):e70012. doi: 10.1002/gcc.70012. Genes Chromosomes Cancer. 2024. PMID: 39565115
-
Management of Resistance to First-Line Anaplastic Lymphoma Kinase Tyrosine Kinase Inhibitor Therapy.Curr Treat Options Oncol. 2018 May 28;19(7):37. doi: 10.1007/s11864-018-0553-x. Curr Treat Options Oncol. 2018. PMID: 29808239 Review.
Cited by
-
Bridging the Divide: A Review on the Implementation of Personalized Cancer Medicine.J Pers Med. 2024 May 24;14(6):561. doi: 10.3390/jpm14060561. J Pers Med. 2024. PMID: 38929782 Free PMC article. Review.
-
Clinical diagnosis and treatment of abdominal inflammatory myofibroblastic tumors.Discov Oncol. 2025 Apr 17;16(1):554. doi: 10.1007/s12672-025-02343-3. Discov Oncol. 2025. PMID: 40244559 Free PMC article.
-
Real-time functional proteomics enhances therapeutic targeting in precision oncology molecular tumor boards.NPJ Precis Oncol. 2025 Apr 15;9(1):111. doi: 10.1038/s41698-025-00868-y. NPJ Precis Oncol. 2025. PMID: 40234655 Free PMC article.
-
Case Report: Primary intracranial high-grade myofibroblastic sarcoma and literature review.Front Oncol. 2025 Apr 2;15:1525401. doi: 10.3389/fonc.2025.1525401. eCollection 2025. Front Oncol. 2025. PMID: 40242239 Free PMC article.
-
Proteomics based selection achieves complete response to HER2 therapy in HER2 IHC 0 breast cancer.NPJ Precis Oncol. 2024 Sep 14;8(1):203. doi: 10.1038/s41698-024-00696-6. NPJ Precis Oncol. 2024. PMID: 39277699 Free PMC article.
References
-
- Griffin CA, Hawkins AL, Dvorak C, et al. . Recurrent involvement of 2p23 in inflammatory myofibroblastic tumors. Cancer Res. 1999;59(12):2776-2780. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
