

Noninvasive Ventilation for Pediatric Acute Respiratory Distress Syndrome: Experience From the 2016/2017 Pediatric Acute Respiratory Distress Syndrome Incidence and Epidemiology Prospective Cohort Study
- PMID: 37255352
- PMCID: PMC10524424
- DOI: 10.1097/PCC.0000000000003281
Noninvasive Ventilation for Pediatric Acute Respiratory Distress Syndrome: Experience From the 2016/2017 Pediatric Acute Respiratory Distress Syndrome Incidence and Epidemiology Prospective Cohort Study
Abstract
Objectives: The worldwide practice and impact of noninvasive ventilation (NIV) in pediatric acute respiratory distress syndrome (PARDS) is unknown. We sought to describe NIV use and associated clinical outcomes in PARDS.
Design: Planned ancillary study to the 2016/2017 prospective Pediatric Acute Respiratory Distress Syndrome Incidence and Epidemiology study.
Setting: One hundred five international PICUs.
Patients: Patients with newly diagnosed PARDS admitted during 10 study weeks.
Interventions: None.
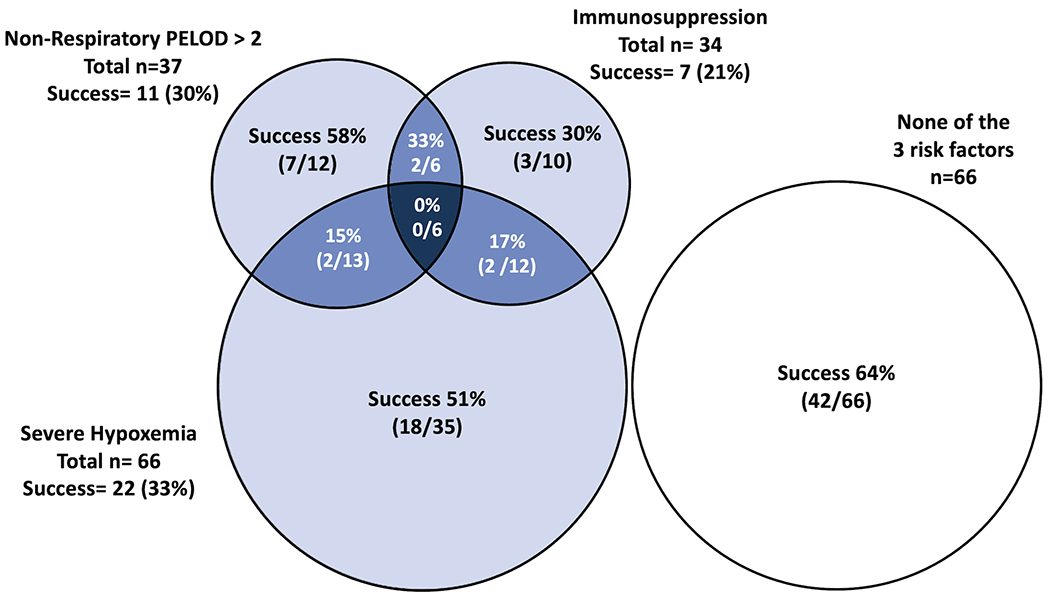
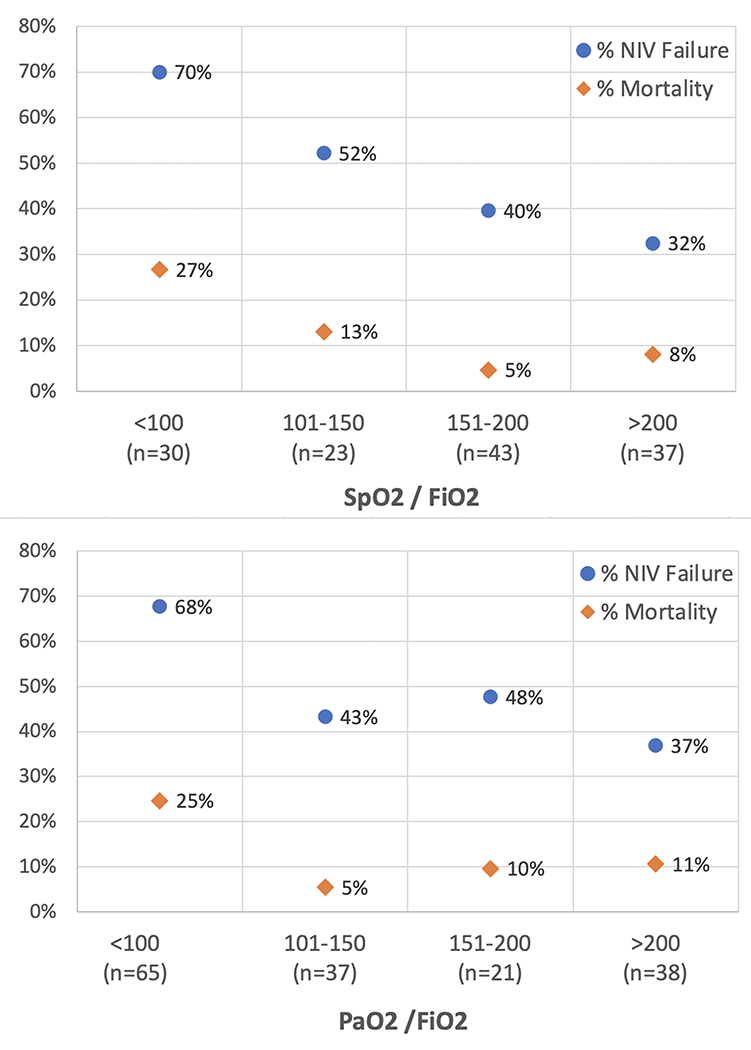
Measurements and main results: Children were categorized by their respiratory support at PARDS diagnosis into NIV or invasive mechanical ventilation (IMV) groups. Of 708 subjects with PARDS, 160 patients (23%) received NIV at PARDS diagnosis (NIV group). NIV failure rate (defined as tracheal intubation or death) was 84 of 160 patients (53%). Higher nonrespiratory pediatric logistic organ dysfunction (PELOD-2) score, Pa o2 /F io2 was less than 100 at PARDS diagnosis, immunosuppression, and male sex were independently associated with NIV failure. NIV failure was 100% among patients with nonrespiratory PELOD-2 score greater than 2, Pa o2 /F io2 less than 100, and immunosuppression all present. Among patients with Pa o2 /F io2 greater than 100, children in the NIV group had shorter total duration of NIV and IMV, than the IMV at initial diagnosis group. We failed to identify associations between NIV use and PICU survival in a multivariable Cox regression analysis (hazard ratio 1.04 [95% CI, 0.61-1.80]) or mortality in a propensity score matched analysis ( p = 0.369).
Conclusions: Use of NIV at PARDS diagnosis was associated with shorter exposure to IMV in children with mild to moderate hypoxemia. Even though risk of NIV failure was high in some children, we failed to identify greater hazard of mortality in these patients.
Copyright © 2023 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Dr. Emeriaud’s institution received funding from Fonds de recherche du Quebec Santé (research public agency award) and Maquet. Dr. Pons-Òdena’s institution received funding from Medtronic; he received funding from Philips Respironics. Drs. Bhalla and Killien received support for article research from the National Institutes of Health. Dr. Shein received funding from Hill Ward Henderson. Dr. Killien’s institution received funding from the National Institutes of Child Health and Human Development. Dr. Rowan’s institution received funding from the National Heart, Lung, and Blood Institute (K23). Dr. Lin received funding from ROMTech. Dr. Napolitano’s institution received funding from Drager, Actuated Medical, Philips/Respinronics, and VeroBiotech. Dr. Khemani received funding from Orange Med and Bayer. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Noninvasive Ventilation in Pediatric Acute Respiratory Distress Syndrome: "Another Dogma Bites the Dust".Pediatr Crit Care Med. 2023 Sep 1;24(9):783-785. doi: 10.1097/PCC.0000000000003299. Epub 2023 Sep 5. Pediatr Crit Care Med. 2023. PMID: 37668500 No abstract available.
References
-
- Wolfler A, Calderini E, Iannella E, et al. Evolution of Noninvasive Mechanical Ventilation Use: A Cohort Study Among Italian PICUs. Pediatr Crit Care Med 2015;16(5):418–427. - PubMed
-
- Mayordomo-Colunga J, Pons-Odena M, Medina A, et al. Non-invasive ventilation practices in children across Europe. Pediatr Pulmonol 2018;53(8):1107–1114. - PubMed
-
- Boghi D, Kim KW, Kim JH, et al. Noninvasive Ventilation for Acute Respiratory Failure in Pediatric Patients: A Systematic Review and Meta-Analysis. Pediatr Crit Care Med 2023;24(2):123–132. - PubMed
-
- Brochard L, Slutsky A, Pesenti A. Mechanical Ventilation to Minimize Progression of Lung Injury in Acute Respiratory Failure. Am J Respir Crit Care Med 2017;195(4):438–442. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
