

Implementation of the measure of case discussion complexity to guide selection of prostate cancer patients for multidisciplinary team meetings
- PMID: 37255390
- PMCID: PMC10417062
- DOI: 10.1002/cam4.6189
Implementation of the measure of case discussion complexity to guide selection of prostate cancer patients for multidisciplinary team meetings
Abstract
Background: Multidisciplinary team meetings (MDTMs) provide an integrated team approach to ensure individualized and evidence-based treatment recommendations and best expert advice in cancer care. A growing number of patients and more complex treatment options challenge MDTM resources and evoke needs for case prioritization. In this process, decision aids could provide streamlining and standardize evaluation of case complexity. We applied the recently developed Measure of Case Discussion Complexity, MeDiC, instrument with the aim to validate its performance in another healthcare setting and diagnostic area as a means to provide cases for full MDTM discussions.
Methods: The 26-item MeDiC instrument evaluates case complexity and was applied to 364 men with newly diagnosed prostate cancer in Sweden. MeDiC scores were generated from individual-level health data and were correlated with clinicopathological parameters, healthcare setting, and the observed clinical case selection for MDTMs.
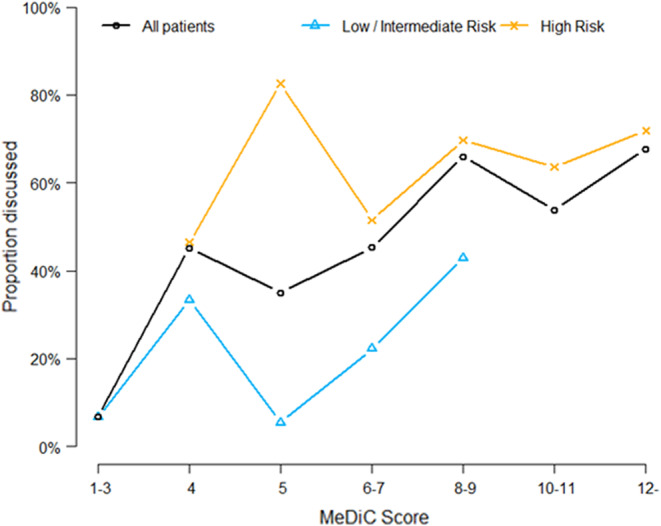
Results: Application of the MeDiC instrument was feasible with rapid scoring based on available clinical data. Patients with high-risk prostate cancers had significantly higher MeDiC scores than patients with low or intermediate-risk cancers. In the total study, population affected lymph nodes and metastatic disease significantly influenced MDTM referral, whereas comorbidities and age did not predict MDTM referral. When individual patient MeDiC scores were compared to the clinical MDTM case selection, advanced stage, T3/T4 tumors, involved lymph nodes, presence of metastases and significant physical comorbidity were identified as key MDTM predictive factors.
Conclusions: Application of the MeDiC instrument in prostate cancer may be used to streamline case selection for MDTMs in cancer care and may complement clinical case selection.
Keywords: comorbidity; decision aid; multidisciplinary team; prostate cancer; tumor board.
© 2023 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


Similar articles
-
Lower MeDiC score is associated with non-referral to multidisciplinary team meeting discussion in bladder cancer patients: a nationwide and population-based study.Acta Oncol. 2025 May 5;64:616-622. doi: 10.2340/1651-226X.2025.42756. Acta Oncol. 2025. PMID: 40325792 Free PMC article.
-
Multicentre evaluation of multidisciplinary team meeting agreement on diagnosis in diffuse parenchymal lung disease: a case-cohort study.Lancet Respir Med. 2016 Jul;4(7):557-565. doi: 10.1016/S2213-2600(16)30033-9. Epub 2016 May 11. Lancet Respir Med. 2016. PMID: 27180021
-
Factors influencing the quality and functioning of oncological multidisciplinary team meetings: results of a systematic review.BMC Health Serv Res. 2022 Jun 27;22(1):829. doi: 10.1186/s12913-022-08112-0. BMC Health Serv Res. 2022. PMID: 35761282 Free PMC article.
-
What is the added value of specialist radiology review of multidisciplinary team meeting cases in a tertiary care center?Eur Radiol. 2024 Oct;34(10):6460-6465. doi: 10.1007/s00330-024-10680-0. Epub 2024 Mar 15. Eur Radiol. 2024. PMID: 38488969 Free PMC article.
-
The Effects of Multidisciplinary Team Meetings on Clinical Practice for Colorectal, Lung, Prostate and Breast Cancer: A Systematic Review.Cancers (Basel). 2021 Aug 18;13(16):4159. doi: 10.3390/cancers13164159. Cancers (Basel). 2021. PMID: 34439312 Free PMC article. Review.
Cited by
-
Implementation of streamlining measures in selecting and prioritising complex cases for the cancer multidisciplinary team meeting: a mini review of the recent developments.Front Health Serv. 2024 Mar 12;4:1340320. doi: 10.3389/frhs.2024.1340320. eCollection 2024. Front Health Serv. 2024. PMID: 38533189 Free PMC article. Review.
-
Interpretation of PSMA-PET Among Urologists: A Prospective Multicentric Evaluation.Cancers (Basel). 2025 Jun 24;17(13):2122. doi: 10.3390/cancers17132122. Cancers (Basel). 2025. PMID: 40647421 Free PMC article.
-
Lower MeDiC score is associated with non-referral to multidisciplinary team meeting discussion in bladder cancer patients: a nationwide and population-based study.Acta Oncol. 2025 May 5;64:616-622. doi: 10.2340/1651-226X.2025.42756. Acta Oncol. 2025. PMID: 40325792 Free PMC article.
References
-
- Soukup T, Lamb BW, Arora S, Darzi A, Sevdalis N, Green JS. Successful strategies in implementing a multidisciplinary team working in the care of patients with cancer: an overview and synthesis of the available literature. J Multidiscip Healthcare. 2018;11:49‐61. doi:10.2147/jmdh.s117945 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
