

The spectrum of COVID-19-associated chorioretinal vasculopathy
- PMID: 37255549
- PMCID: PMC10193817
- DOI: 10.1016/j.ajoc.2023.101857
The spectrum of COVID-19-associated chorioretinal vasculopathy
Abstract
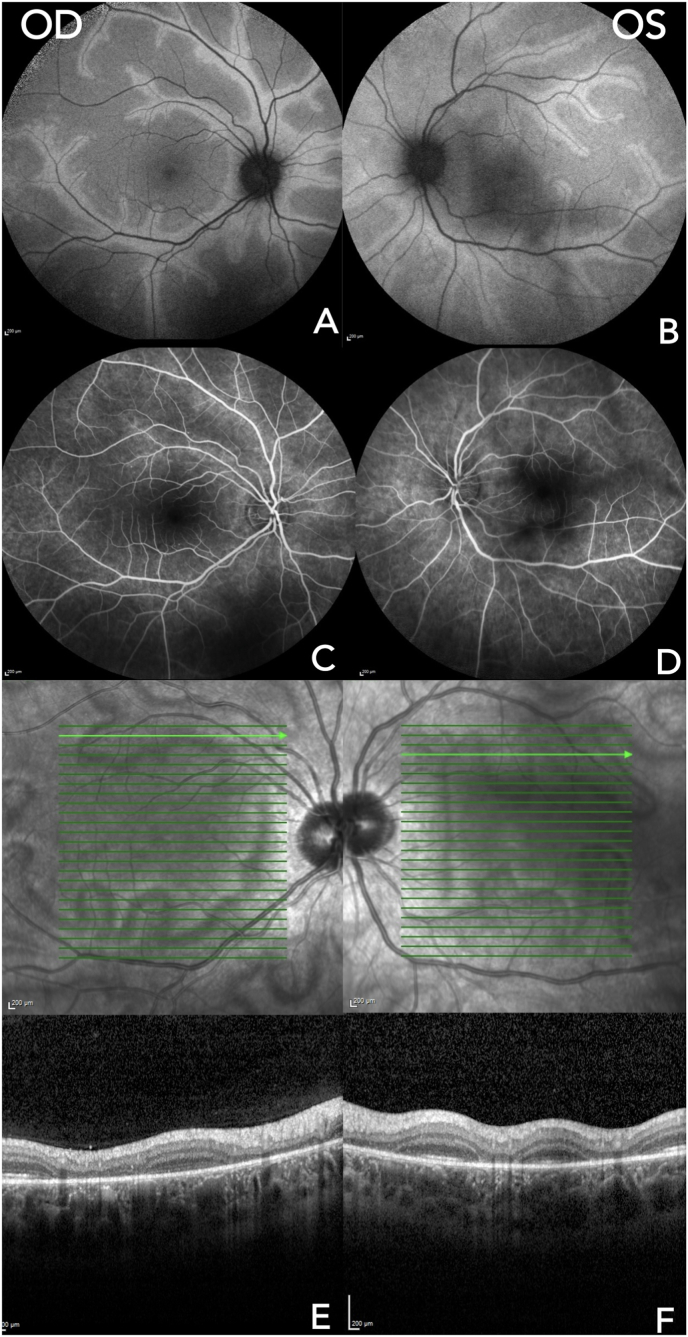
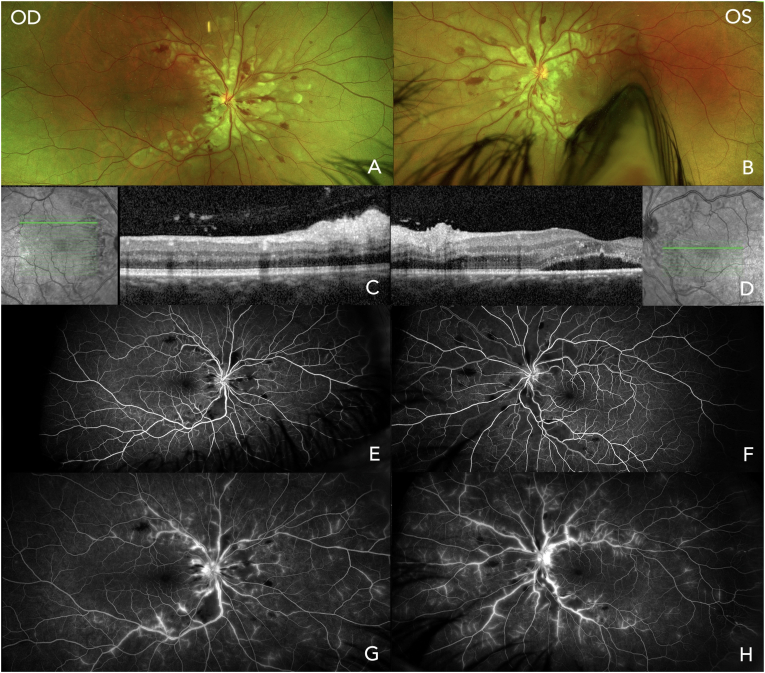
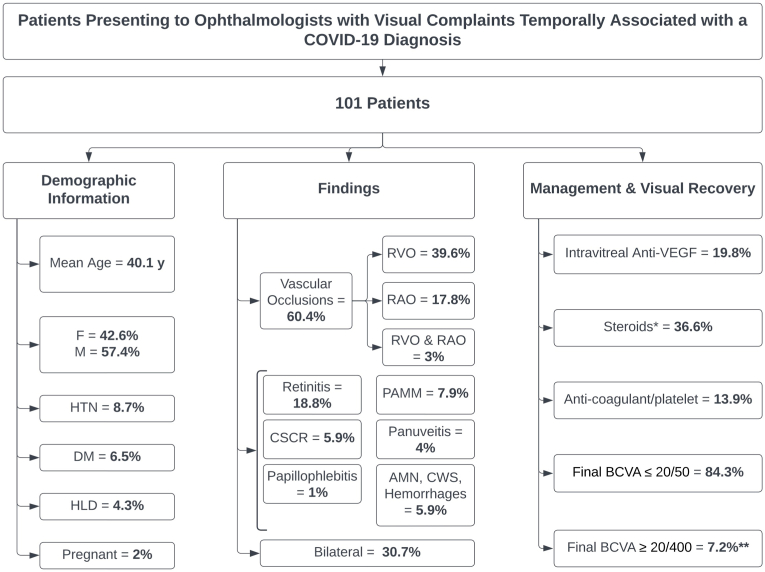
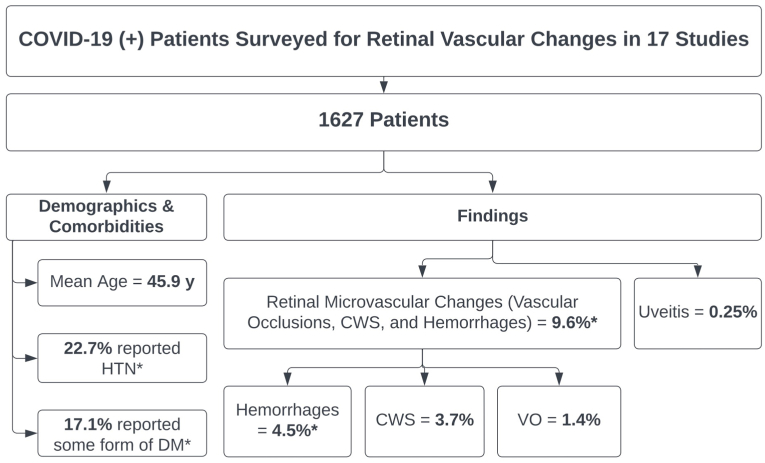
Purpose: Although conjunctivitis represents the most common ocular manifestation of COVID-19 infection, sight-threatening retinal involvement has been reported. Herein, we report and characterize with multimodal retinal imaging 5 cases of acute vision loss secondary to presumed chorioretinal vasculopathy temporally associated with COVID-19 infection with varying severity, visual morbidity, and treatment response, and review the available literature on the association between COVID-19 infection and retinal microvascular changes.
Design: Observational case series and literature review.
Methods: Multicenter case series of 5 patients who presented to academic centers and private offices with acute vision loss temporally associated with COVID-19 infection. A review of the literature was conducted using online databases.
Results: 10 eyes of 5 patients, 3 men and 2 women, with a mean age of 30.8 years (median 33, range 16-44) were described. All patients had a recently preceding episode of COVID-19, with symptomatology ranging from mild infection to life-threatening encephalopathy. Treatment for their retinal disease included topical, oral, intravitreal, and intravenous steroids, steroid-sparing immunosuppression, retinal photocoagulation, antivirals, and antiplatelet and anticoagulant agents. Treatment response and visual recovery ranged from complete recovery of baseline acuity to permanent vision loss and need for chronic immunosuppression.
Conclusions and importance: Clinicians should be mindful of the potential for vision-threatening retinal involvement after COVID-19 infection. If found, treatment with both anti-inflammatory therapy and anticoagulation should be considered, in addition to close monitoring, as some patients with this spectrum of disease may require chronic immune suppression and/or anti-VEGF therapy.
Keywords: COVID-19; Chorioretinal vasculopathy; Retinal microvascular changes.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
