

aMplitude spectral area of ventricular fibrillation and amiOdarone Study in patients with out-of-hospital cArdIaC arrest. The MOSAIC study
- PMID: 37255711
- PMCID: PMC10226588
- DOI: 10.3389/fcvm.2023.1179815
aMplitude spectral area of ventricular fibrillation and amiOdarone Study in patients with out-of-hospital cArdIaC arrest. The MOSAIC study
Abstract
Objective: Antiarrhythmic drugs are recommended for out of hospital cardiac arrest (OHCA) with shock-refractory ventricular fibrillation (VF). Amplitude Spectral Area (AMSA) of VF is a quantitative waveform measure that describes the amplitude-weighted mean frequency of VF, it correlates with intramyocardial adenosine triphosphate (ATP) concentration, it is a predictor of shock efficacy and an emerging indicator to guide defibrillation and resuscitation efforts. How AMSA might be influenced by amiodarone administration is unknown.
Methods: In this international multicentre observational study, all OHCAs receiving at least one shock were included. AMSA values were calculated by retrospectively analysing the pre-shock ECG interval of 2 s. Multivariable models were run and a propensity score based on the probability of receiving amiodarone was created to compare two randomly matched samples.
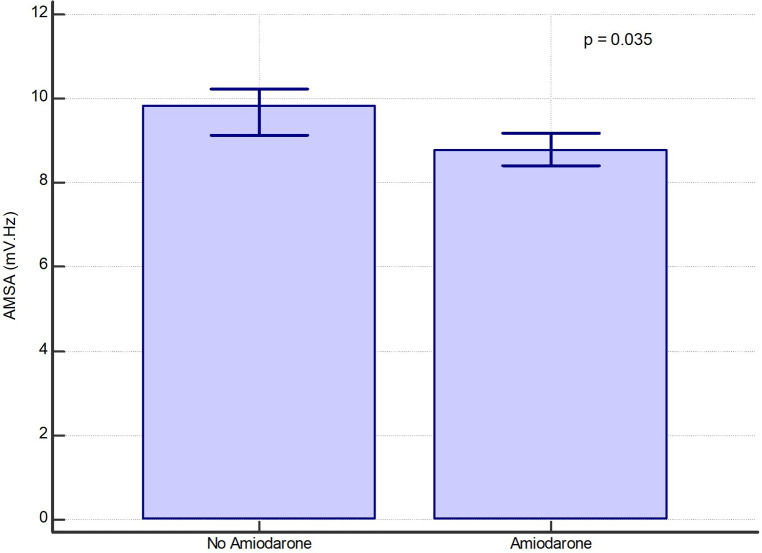
Results: 2,077 shocks were included: 1,407 in the amiodarone group and 670 in the non-amiodarone group. AMSA values were lower in the amiodarone group [8.8 (6-12.7) mV·Hz vs. 9.8 (6-14) mV·Hz, p = 0.035]. In two randomly matched propensity score-based groups of 261 shocks, AMSA was lower in the amiodarone group [8.2 (5.8-13.5) mV·Hz vs. 9.6 (5.6-11.6), p = 0.042]. AMSA was a predictor of shock success in both groups but the predictive power was lower in the amiodarone group [Area Under the Curve (AUC) non-amiodarone group 0.812, 95%CI: 0.78-0.841 vs. AUC amiodarone group 0.706, 95%CI: 0.68-0.73; p < 0.001].
Conclusions: Amiodarone administration was independently associated with the probability of recording lower values of AMSA. In patients who have received amiodarone during cardiac arrest the predictive value of AMSA for shock success is significantly lower, but still statistically significant.
Keywords: AMSA; amidoarone; cardiac arrest; defibrillation; ventricular fibrillation.
© 2023 Gentile, Wik, Aramendi, Baldi, Isasi, Steen-Hansen, Compagnoni, Fasolino, Contri, Palo, Primi, Bendotti, Currao and Savastano.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Berg KM, Soar J, Andersen LW, Böttiger BW, Cacciola S, Callaway CW, et al. Adult advanced life support: 2020 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. (2020) 142:92–139. 10.1161/CIRCULATIONAHA.120.045957 - DOI - PubMed
-
- Panchal AR, Berg KM, Kudenchuk PJ, Del Rios M, Hirsch KG, Link MS, et al. 2018 American heart association focused update on advanced cardiovascular life support use of antiarrhythmic drugs during and immediately after cardiac arrest: an update to the American heart association guidelines for cardiopulmonary resuscitation and Em. Circulation (2018) 138(23):e740–9. 10.1161/CIR.0000000000000613 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources