

High-dose ubiquinol supplementation in multiple-system atrophy: a multicentre, randomised, double-blinded, placebo-controlled phase 2 trial
- PMID: 37256098
- PMCID: PMC10225719
- DOI: 10.1016/j.eclinm.2023.101920
High-dose ubiquinol supplementation in multiple-system atrophy: a multicentre, randomised, double-blinded, placebo-controlled phase 2 trial
Abstract
Background: Functionally impaired variants of COQ2, encoding an enzyme in biosynthesis of coenzyme Q10 (CoQ10), were found in familial multiple system atrophy (MSA) and V393A in COQ2 is associated with sporadic MSA. Furthermore, reduced levels of CoQ10 have been demonstrated in MSA patients.
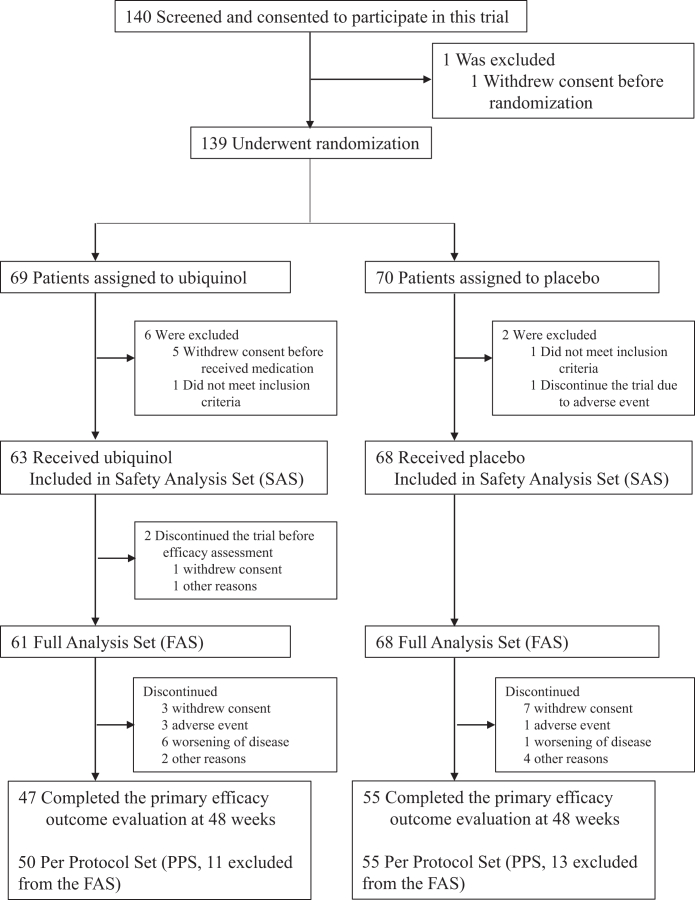
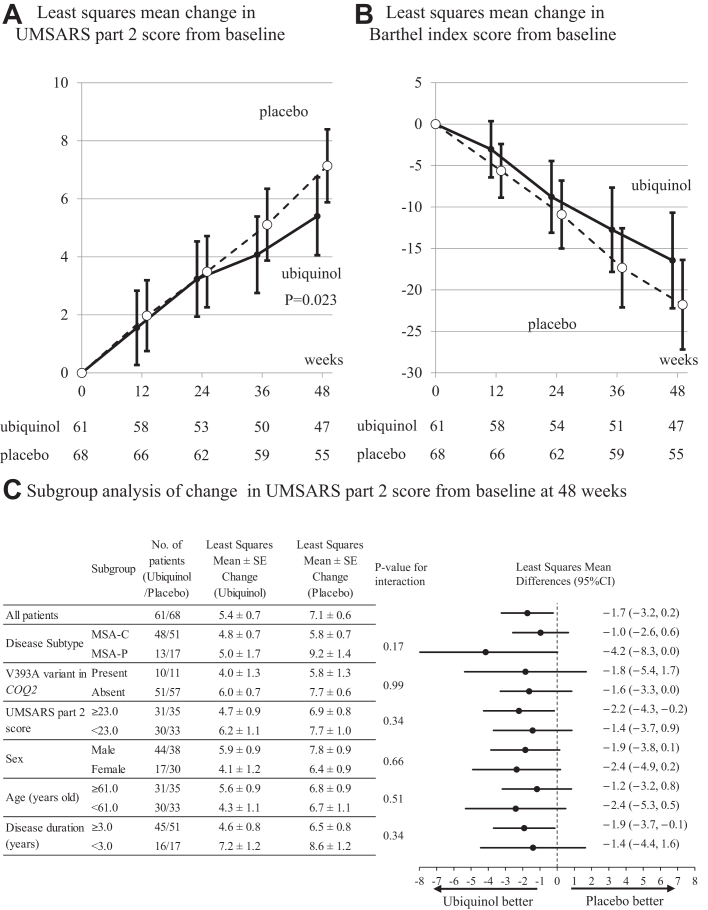
Methods: This study was a multicentre, randomised, double-blinded, placebo-controlled phase 2 trial. Patients with MSA were randomly assigned (1:1) to either ubiquinol (1500 mg/day) or placebo. The primary efficacy outcome was the change in the unified multiple system atrophy rating scale (UMSARS) part 2 at 48 weeks. Efficacy was assessed in all patients who completed at least one efficacy assessment (full analysis set). Safety analyses included patients who completed at least one dose of investigational drug. This trial is registered with UMIN-CTR (UMIN000031771), where the drug name of MSA-01 was used to designate ubiquinol.
Findings: Between June 26, 2018, and May 27, 2019, 139 patients were enrolled and randomly assigned to the ubiquinol group (n = 69) or the placebo group (n = 70). A total of 131 patients were included in the full analysis set (63 in the ubiquinol group; 68 in the placebo group). This study met the primary efficacy outcome (least square mean difference in UMSARS part 2 score (-1.7 [95% CI, -3.2 to -0.2]; P = 0.023)). The ubiquinol group also showed better secondary efficacy outcomes (Barthel index, Scale for the Assessment and Rating of Ataxia, and time required to walk 10 m). Rates of adverse events potentially related to the investigational drug were comparable between ubiquinol (n = 15 [23.8%]) and placebo (n = 21 [30.9%]).
Interpretation: High-dose ubiquinol was well-tolerated and led to a significantly smaller decline of UMSARS part 2 score compared with placebo.
Funding: Japan Agency for Medical Research and Development.
Keywords: COQ2; Clinical trial; Disease-modifying therapy; Multiple system atrophy; Ubiquinol.
© 2023 The Author(s).
Conflict of interest statement
JM reports honoraria from Kyowa Kirin, Alnylam Japan, Sanofi, Sumitomo Pharma, Pfizer, Daiichi Sankyo, and Takeda Pharmaceutical Company; grants from Japan Agency for Medical Research and Development (AMED), Japan Society for the Promotion of Science (JSPS), and Takeda Science Foundation. TM reports honoraria from Eisai and Sumitomo Pharma; grants from JSPS. HI reports honoraria from Takeda Pharmaceutical Company, Eisai, Biogen Japan, Sumitomo Pharma, FP Pharmaceutical Corporation, Kyowa Kirin, UCB Japan, Chugai Pharmaceutical, and Daiichi Sankyo Company; grants from AMED, JSPS, and Kato Memorial Trust for Nanbyo Research. TT reports honoraria from Sumitomo Pharma. OO reports honoraria from Kyowa Hakko Kirin Co., Ltd., Bristol-Myers Squibb, Ono Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharm, Takeda, Daiichi-Sankyo, FUJIFILM, SANOFI, and FP-pharm; grants from AMED, JSPS, Japanese Ministry of Health, Labor, and Welfare, Takeda Science Foundation, and Life Science Foundation of Japan. ST reports consulting fees from Sanwakagaku Kenkyusho, and Ono Pharmaceutical; honoraria from Sanofi, Senju Pharmaceutical, Novartis, Kyowa Kirin, and Daiichisankyo; grants from AMED, JSPS, and Nobel Pharma. All other authors declare no competing interests.
Figures
References
-
- Fanciulli A., Wenning G.K. Multiple-system atrophy. N Engl J Med. 2015;372:249–263. - PubMed
-
- Watanabe H., Saito Y., Terao S., et al. Progression and prognosis in multiple system atrophy: an analysis of 230 Japanese patients. Brain. 2002;125:1070–1083. - PubMed
-
- Wakabayashi K., Yoshimoto M., Tsuji S., Takahashi H. Alpha-synuclein immunoreactivity in glial cytoplasmic inclusions in multiple system atrophy. Neurosci Lett. 1998;249:180–182. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
