

Association Between Mobilization and Composite Postoperative Complications Following Major Elective Surgery
- PMID: 37256591
- PMCID: PMC10233451
- DOI: 10.1001/jamasurg.2023.1122
Association Between Mobilization and Composite Postoperative Complications Following Major Elective Surgery
Abstract
Importance: Mobilization after surgery is a key component of Enhanced Recovery after Surgery (ERAS) pathways.
Objective: To evaluate the association between mobilization and a collapsed composite of postoperative complications in patients recovering from major elective surgery as well as hospital length of stay, cumulative pain scores, and 30-day readmission rates.
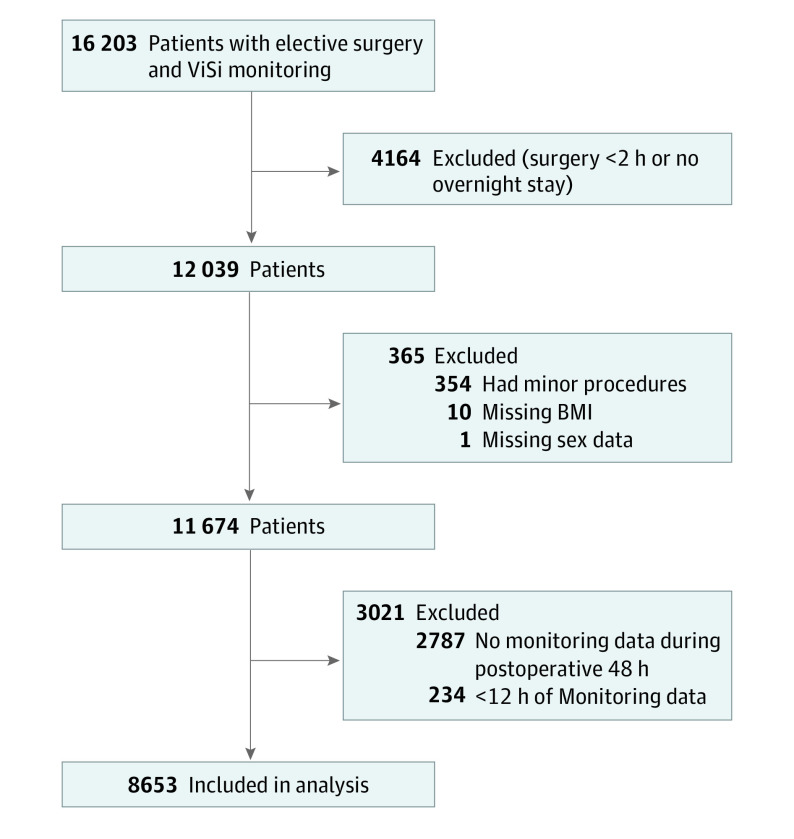
Design, setting, and participants: This retrospective observational study conducted at a single quaternary US referral center included patients who had elective surgery between February 2017 and October 2020. Mobilization was assessed over the first 48 postoperative hours with wearable accelerometers, and outcomes were assessed throughout hospitalization. Patients who had elective surgery lasting at least 2 hours followed by at least 48 hours of hospitalization were included. A minimum of 12 hours of continuous accelerometer monitoring was required without missing confounding variables or key data. Among 16 203 potential participants, 8653 who met inclusion criteria were included in the final analysis. Data were analyzed from February 2017 to October 2020.
Exposures: Amount of mobilization per hour for 48 postoperative hours.
Outcomes: The primary outcome was a composite of myocardial injury, ileus, stroke, venous thromboembolism, pulmonary complications, and all-cause in-hospital mortality. Secondary outcomes included hospital length of stay, cumulative pain scores, and 30-day readmission.
Results: Of 8653 included patients (mean [SD] age, 57.6 [16.0] years; 4535 [52.4%] female), 633 (7.3%) experienced the primary outcome. Mobilization time was a median (IQR) of 3.9 (1.7-7.8) minutes per monitored hour overall, 3.2 (0.9-7.4) in patients who experienced the primary outcome, and 4.1 (1.8-7.9) in those who did not. There was a significant association between postoperative mobilization and the composite outcome (hazard ratio [HR], 0.75; 95% CI, 0.67-0.84; P < .001) for each 4-minute increase in mobilization. Mobilization was associated with an estimated median reduction in the duration of hospitalization by 0.12 days (95% CI, 0.09-0.15; P < .001) for each 4-minute increase in mobilization. The were no associations between mobilization and pain score or 30-day readmission.
Conclusions and relevance: In this study, mobilization measured by wearable accelerometers was associated with fewer postoperative complications and shorter hospital length of stay.
Conflict of interest statement
Figures
Comment in
-
Mobilization and Composite Postoperative Complications.JAMA Surg. 2023 Aug 1;158(8):831. doi: 10.1001/jamasurg.2023.1128. JAMA Surg. 2023. PMID: 37256595 No abstract available.
-
Mobilization, Just 1 Component of Enhanced Recovery After Surgery.JAMA Surg. 2024 Feb 1;159(2):230-231. doi: 10.1001/jamasurg.2023.5230. JAMA Surg. 2024. PMID: 37938832 No abstract available.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
