

Late-onset Cognitive Impairment and Modifiable Risk Factors in Adult Childhood Cancer Survivors
- PMID: 37256617
- PMCID: PMC10233416
- DOI: 10.1001/jamanetworkopen.2023.16077
Late-onset Cognitive Impairment and Modifiable Risk Factors in Adult Childhood Cancer Survivors
Abstract
Importance: Long-term survivors of childhood cancer may be at elevated risk for new neurocognitive impairment and decline as they age into adulthood.
Objective: To determine whether aging adult childhood cancer survivors report more new-onset neurocognitive impairments compared with their siblings and to identify risk factors associated with such impairments.
Design, setting, and participants: Participants of this cohort study included adult survivors of childhood cancer from the Childhood Cancer Survivor Study and their siblings as a control group. The original cohort included survivors who received a diagnosis between January 1, 1970, and December 31, 1986, for whom longitudinal neurocognitive assessment was available. This study examined the prevalence of new-onset neurocognitive impairment between baseline (23.4 years after diagnosis) and follow-up (35.0 years after diagnosis). The analysis was performed from January 2021 to May 2022.
Exposures: Cancer treatment exposures were abstracted from medical records. Chronic health conditions were graded using Common Terminology Criteria for Adverse Events version 4.03.
Main outcomes and measures: The primary outcome was new-onset (present at follow-up, but not present at baseline) neurocognitive impairment (defined as a score in the worst 10% of the sibling cohort). Impairment was assessed using the Childhood Cancer Survivor Study Neurocognitive questionnaire. Relative risks (RRs) and 95% CIs were used to estimate associations of neurocognitive impairment with treatment and health behaviors and conditions using generalized linear models.
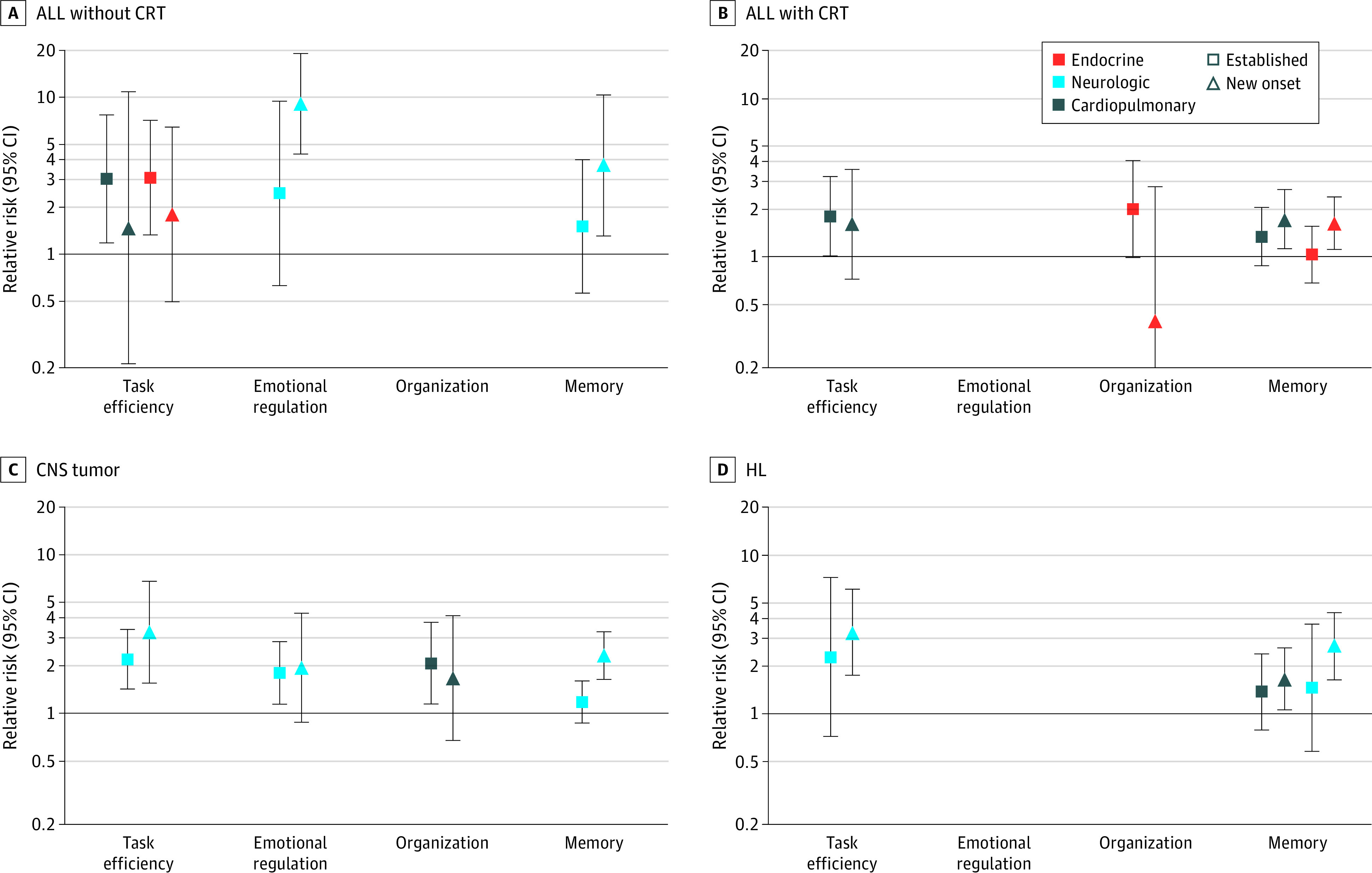
Results: The cohort comprised 2375 survivors (mean [SD] age at evaluation, 31.8 [7.5] years; 1298 women [54.6%]) of childhood cancer, including acute lymphoblastic leukemia (ALL; 1316 participants), central nervous system (CNS) tumors (488 participants), and Hodgkin lymphoma (HL; 571 participants). A total of 232 siblings (mean [SD] age at evaluation, 34.2 [8.4] years; 134 women [57.8%]) were included. Compared with siblings, a higher proportion of survivors with no impairment in memory at baseline had new-onset memory impairment at follow-up: siblings proportion, 7.8% (95% CI, 4.3%-11.4%); ALL survivors treated with chemotherapy only, 14.0% (95% CI, 10.7%-17.4%); ALL survivors treated with cranial radiation (CRT), 25.8% (95% CI, 22.6%-29.0%); CNS tumor survivors, 34.7% (95% CI, 30.0%-39.5%); and HL survivors, 16.6% (95% CI, 13.4%-19.8%). New-onset memory impairment was associated with CRT in CNS tumor survivors (RR, 1.97; 95% CI, 1.33-2.90) and alkylator chemotherapy greater than or equal to 8000 mg/m2 in ALL survivors treated without CRT (RR, 2.80; 95% CI, 1.28-6.12). Neurologic conditions mediated the impact of CRT on new-onset memory impairment in CNS survivors. Smoking, low educational attainment, and low physical activity were associated with elevated risk for new-onset memory impairment.
Conclusions and relevance: These findings suggest that adult survivors of childhood cancer are at elevated risk for late-onset memory impairment related to modifiable risk factors identified early in survivorship.
Conflict of interest statement
Figures


References
-
- Gibson TM, Mostoufi-Moab S, Stratton KL, et al. . Temporal patterns in the risk of chronic health conditions in survivors of childhood cancer diagnosed 1970-99: a report from the Childhood Cancer Survivor Study cohort. Lancet Oncol. 2018;19(12):1590-1601. doi:10.1016/S1470-2045(18)30537-0 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
