

Comparison of Cystatin C and Creatinine in the Assessment of Measured Kidney Function during Critical Illness
- PMID: 37256861
- PMCID: PMC10564373
- DOI: 10.2215/CJN.0000000000000203
Comparison of Cystatin C and Creatinine in the Assessment of Measured Kidney Function during Critical Illness
Abstract
Background: Incomplete recovery of kidney function is an important adverse outcome in survivors of critical illness. However, unlike eGFR creatinine, eGFR cystatin C is not confounded by muscle loss and may improve identification of persistent kidney dysfunction.
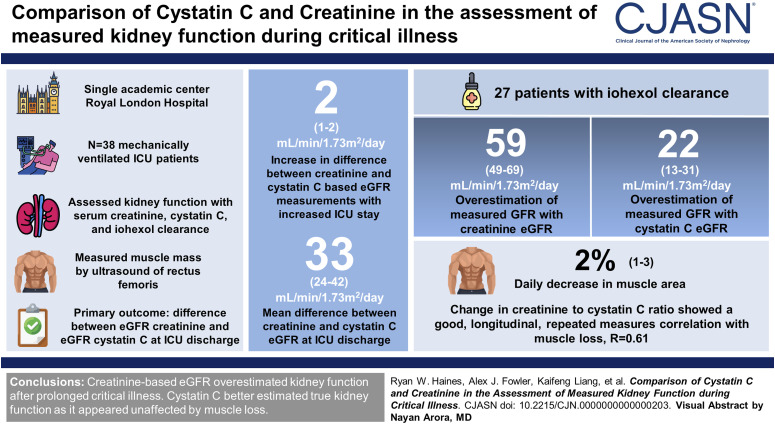
Methods: To assess kidney function during prolonged critical illness, we enrolled 38 mechanically ventilated patients with an expected length of stay of >72 hours near admission to intensive care unit (ICU) in a single academic medical center. We assessed sequential kidney function using creatinine, cystatin C, and iohexol clearance measurements. The primary outcome was difference between eGFR creatinine and eGFR cystatin C at ICU discharge using Bayesian regression modeling. We simultaneously measured muscle mass by ultrasound of the rectus femoris to assess the confounding effect on serum creatinine generation.
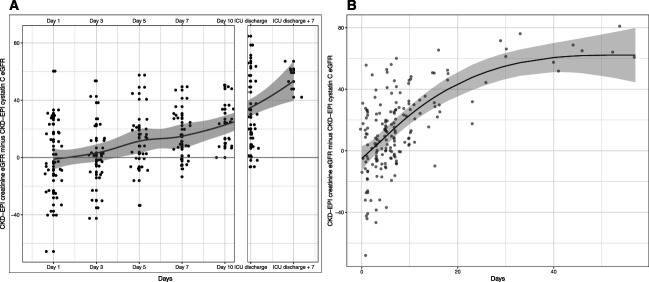
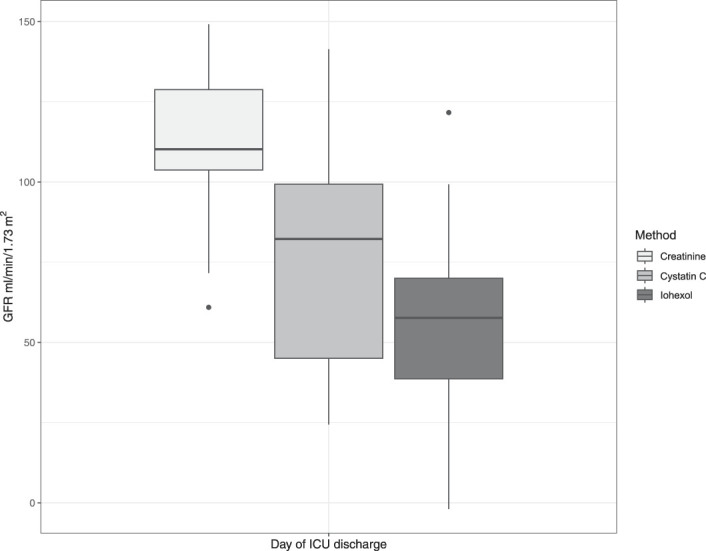
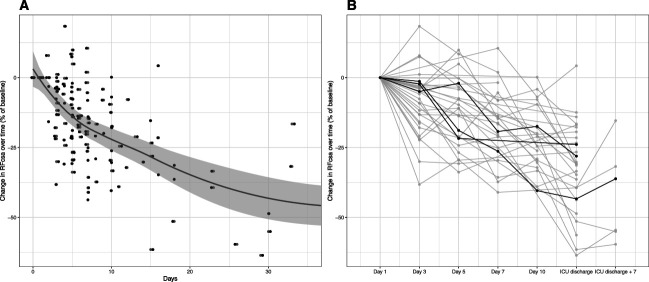
Results: Longer length of ICU stay was associated with greater difference between eGFR creatinine and eGFR cystatin C at a predicted rate of 2 ml/min per 1.73 m 2 per day (95% confidence interval [CI], 1 to 2). By ICU discharge, the posterior mean difference between creatinine and cystatin C eGFR was 33 ml/min per 1.73 m 2 (95% credible interval [CrI], 24 to 42). In 27 patients with iohexol clearance measured close to ICU discharge, eGFR creatinine was on average two-fold greater than the iohexol gold standard, and posterior mean difference was 59 ml/min per 1.73 m 2 (95% CrI, 49 to 69). The posterior mean for eGFR cystatin C suggested a 22 ml/min per 1.73 m 2 (95% CrI, 13 to 31) overestimation of measured GFR. Each day in ICU resulted in a predicted 2% (95% CI, 1% to 3%) decrease in muscle area. Change in creatinine-to-cystatin C ratio showed good longitudinal, repeated measures correlation with muscle loss, R =0.61 (95% CI, 0.50 to 0.72).
Conclusions: eGFR creatinine systematically overestimated kidney function after prolonged critical illness. Cystatin C better estimated true kidney function because it seemed unaffected by the muscle loss from prolonged critical illness.
Clinical trial registry name and registration number: Skeletal Muscle Wasting and Renal Dysfunction After Critical Illness Trauma - Outcomes Study (KRATOS), NCT03736005 .
Copyright © 2023 by the American Society of Nephrology.
Conflict of interest statement
A.J. Fowler reports research funding from Barts Charity and National Institutes of Health Research. R.M. Pearse reports employment with Bart Health NHS Trust; research funding from Edwards Life Sciences, GlaxoSmithKline, and Intersurgical; and honoraria from Edwards Life Sciences, GlaxoSmithKline, and Intersurgical. J.R. Prowle reports employment with Barts Health NHS Trust; consultancy for Baxter, Nikkiso Europe, Jafron Biomedical Co Ltd, Mission Therapeutics Ltd, Cambridge UK, Nephrolytx GmbH, and Paion Ltd; research funding from Barts and the London Charity, bioMérieux SA, Jafron Biomedical Ltd, National Institue of Health Research, and Rosetrees Trust; honoraria from Baxter Inc, BBraun, Fresenius Kabi, and Nikkiso Europe GmbH; a US patent application “Markers of Acute Kidney Injury” in conjunction with Dr M. Westerman, Intrinsic LifeSciences LLC, La Jolla, CA, USA; and other interests or relationships as UK Kidney Research Consortium (UKKRC) Acute Kidney Injury Clinical Specialties Group colead and European Society of Intensive Care Medicine Acute Kidney Injury Speciality Section Chair Elect. Z. Puthucheary reports employment with Puthucheary Medical Consultancy Ltd; consultancy for Bioage, Faraday Pharmaceuticals, Fresenius Kabi, Nestle, and Nutricia; ownership interest in Puthucheary Medical Consultancy Ltd; research funding from Baxter, Fresenius Kabi, and Vitaflo (Nestle); and honoraria from Baxter, Sedana, Fresenius Kabi, Nestle, and Nutricia. All remaining authors have nothing to disclose.
Figures
Comment in
-
Should We Really Still Be Using Creatinine in the Critical Care Setting?Clin J Am Soc Nephrol. 2023 Aug 1;18(8):988-990. doi: 10.2215/CJN.0000000000000225. Epub 2023 Jul 5. Clin J Am Soc Nephrol. 2023. PMID: 37410991 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
