

Capivasertib in Hormone Receptor-Positive Advanced Breast Cancer
- PMID: 37256976
- PMCID: PMC11335038
- DOI: 10.1056/NEJMoa2214131
Capivasertib in Hormone Receptor-Positive Advanced Breast Cancer
Abstract
Background: AKT pathway activation is implicated in endocrine-therapy resistance. Data on the efficacy and safety of the AKT inhibitor capivasertib, as an addition to fulvestrant therapy, in patients with hormone receptor-positive advanced breast cancer are limited.
Methods: In a phase 3, randomized, double-blind trial, we enrolled eligible pre-, peri-, and postmenopausal women and men with hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer who had had a relapse or disease progression during or after treatment with an aromatase inhibitor, with or without previous cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitor therapy. Patients were randomly assigned in a 1:1 ratio to receive capivasertib plus fulvestrant or placebo plus fulvestrant. The dual primary end point was investigator-assessed progression-free survival assessed both in the overall population and among patients with AKT pathway-altered (PIK3CA, AKT1, or PTEN) tumors. Safety was assessed.
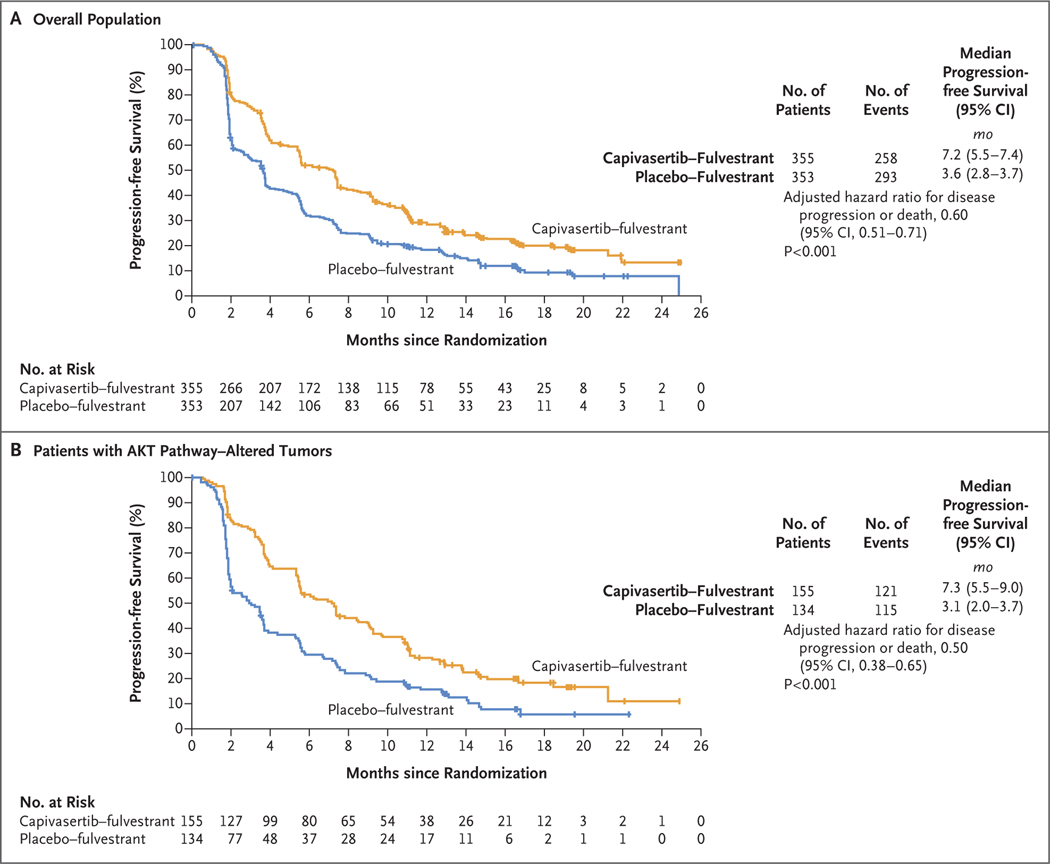
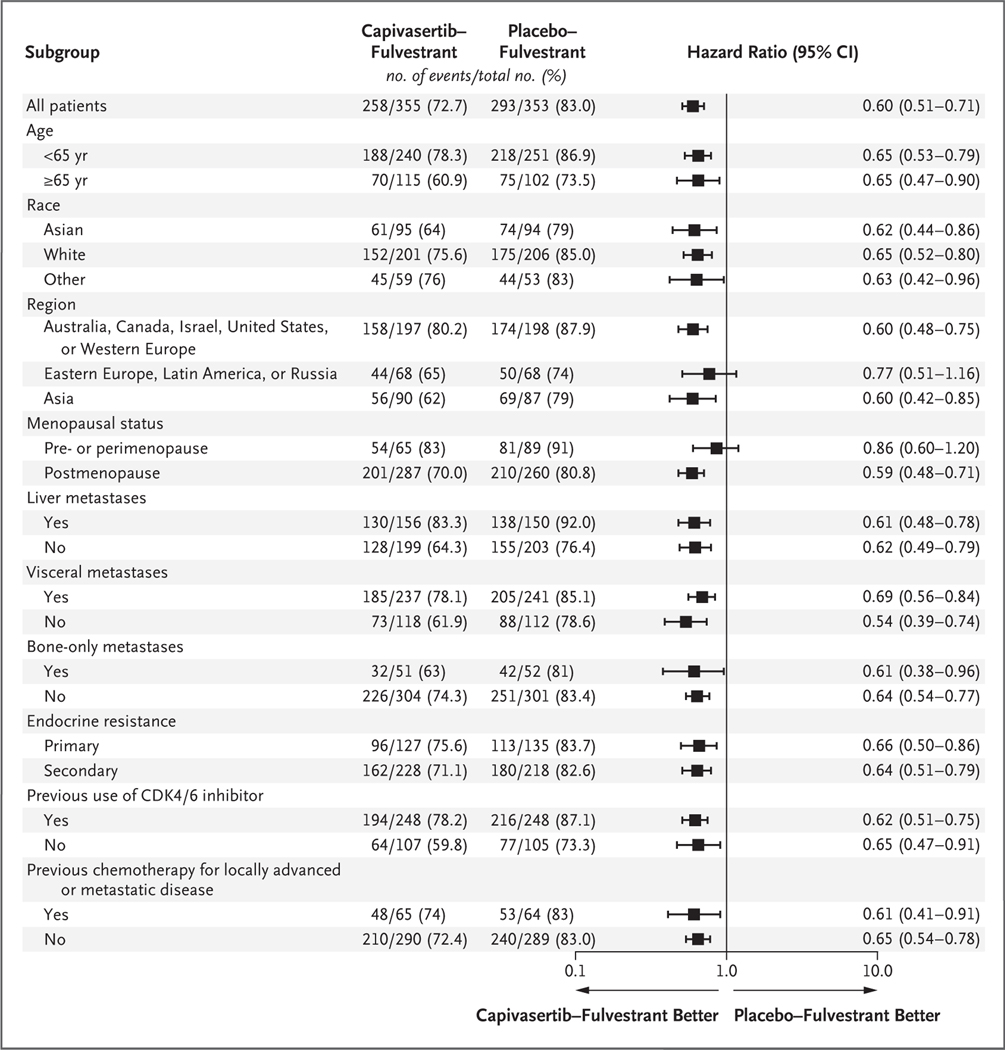
Results: Overall, 708 patients underwent randomization; 289 patients (40.8%) had AKT pathway alterations, and 489 (69.1%) had received a CDK4/6 inhibitor previously for advanced breast cancer. In the overall population, the median progression-free survival was 7.2 months in the capivasertib-fulvestrant group, as compared with 3.6 months in the placebo-fulvestrant group (hazard ratio for progression or death, 0.60; 95% confidence interval [CI], 0.51 to 0.71; P<0.001). In the AKT pathway-altered population, the median progression-free survival was 7.3 months in the capivasertib-fulvestrant group, as compared with 3.1 months in the placebo-fulvestrant group (hazard ratio, 0.50; 95% CI, 0.38 to 0.65; P<0.001). The most frequent adverse events of grade 3 or higher in patients receiving capivasertib-fulvestrant were rash (in 12.1% of patients, vs. in 0.3% of those receiving placebo-fulvestrant) and diarrhea (in 9.3% vs. 0.3%). Adverse events leading to discontinuation were reported in 13.0% of the patients receiving capivasertib and in 2.3% of those receiving placebo.
Conclusions: Capivasertib-fulvestrant therapy resulted in significantly longer progression-free survival than treatment with fulvestrant alone among patients with hormone receptor-positive advanced breast cancer whose disease had progressed during or after previous aromatase inhibitor therapy with or without a CDK4/6 inhibitor. (Funded by AstraZeneca and the National Cancer Institute; CAPItello-291 ClinicalTrials.gov number, NCT04305496.).
Copyright © 2023 Massachusetts Medical Society.
Figures
References
-
- Gennari A, André F, Barrios CH, et al. ESMO clinical practice guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann Oncol 2021; 32: 1475–95. - PubMed
-
- National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology (NCCN Guidelines): breast cancer (version 4.2022).
-
- Millis SZ, Ikeda S, Reddy S, Gatalica Z, Kurzrock R. Landscape of phosphatidylinositol-3-kinase pathway alterations across 19784 diverse solid tumors. JAMA Oncol 2016; 2: 1565–73. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous