

Mechanical bowel preparation and antibiotics in elective colorectal surgery: network meta-analysis
- PMID: 37257059
- PMCID: PMC10231808
- DOI: 10.1093/bjsopen/zrad040
Mechanical bowel preparation and antibiotics in elective colorectal surgery: network meta-analysis
Abstract
Background: The use of intravenous antibiotics at anaesthetic induction in colorectal surgery is the standard of care. However, the role of mechanical bowel preparation, enemas, and oral antibiotics in surgical site infection, anastomotic leak, and other perioperative outcomes remains controversial. The aim of this study was to determine the optimal preoperative bowel preparation strategy in elective colorectal surgery.
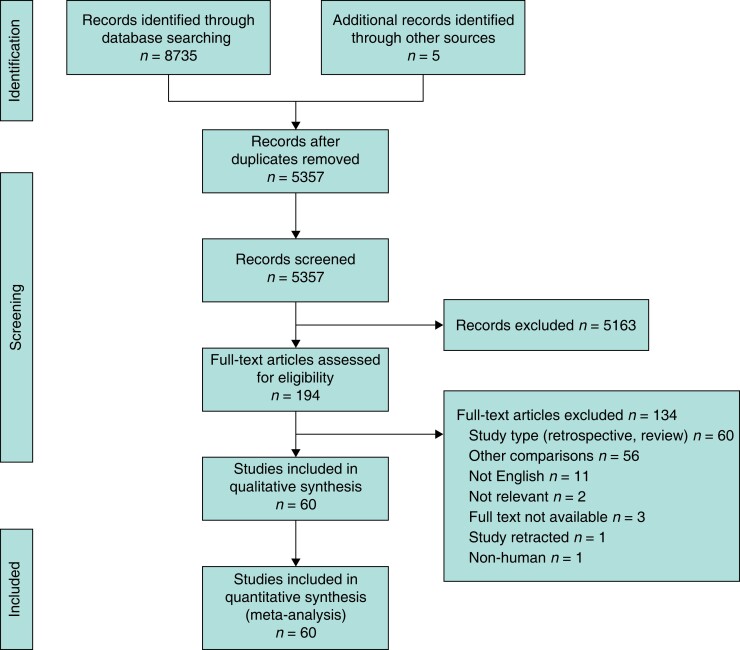
Methods: A systematic review and network meta-analysis of RCTs was performed with searches from PubMed/MEDLINE, Scopus, Embase, and the Cochrane Central Register of Controlled Trials from inception to December 2022. Primary outcomes included surgical site infection and anastomotic leak. Secondary outcomes included 30-day mortality rate, ileus, length of stay, return to theatre, other infections, and side effects of antibiotic therapy or bowel preparation.
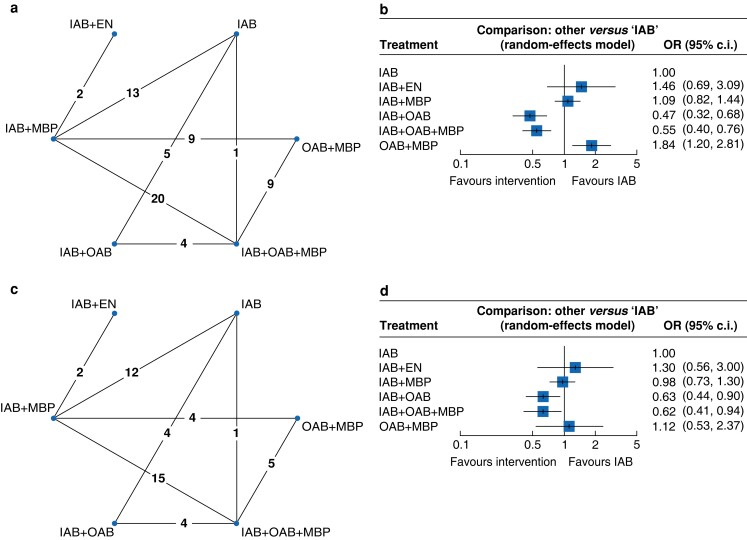
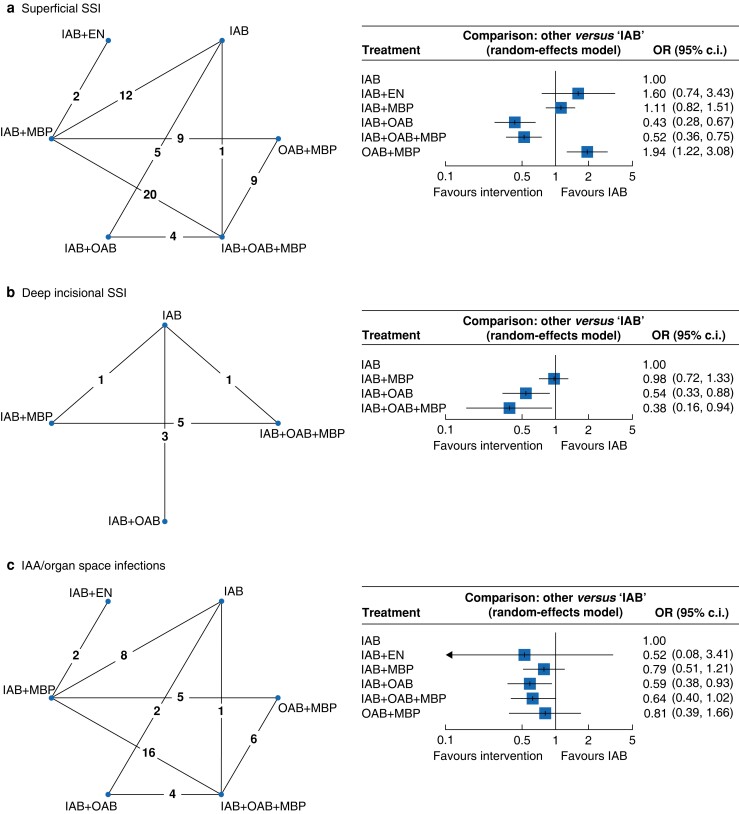
Results: Sixty RCTs involving 16 314 patients were included in the final analysis: 3465 (21.2 per cent) had intravenous antibiotics alone, 5268 (32.3 per cent) had intravenous antibiotics + mechanical bowel preparation, 1710 (10.5 per cent) had intravenous antibiotics + oral antibiotics, 4183 (25.6 per cent) had intravenous antibiotics + oral antibiotics + mechanical bowel preparation, 262 (1.6 per cent) had intravenous antibiotics + enemas, and 1426 (8.7 per cent) had oral antibiotics + mechanical bowel preparation. With intravenous antibiotics as a baseline comparator, network meta-analysis demonstrated a significant reduction in total surgical site infection risk with intravenous antibiotics + oral antibiotics (OR 0.47 (95 per cent c.i. 0.32 to 0.68)) and intravenous antibiotics + oral antibiotics + mechanical bowel preparation (OR 0.55 (95 per cent c.i. 0.40 to 0.76)), whereas oral antibiotics + mechanical bowel preparation resulted in a higher surgical site infection rate compared with intravenous antibiotics alone (OR 1.84 (95 per cent c.i. 1.20 to 2.81)). Anastomotic leak rates were lower with intravenous antibiotics + oral antibiotics (OR 0.63 (95 per cent c.i. 0.44 to 0.90)) and intravenous antibiotics + oral antibiotics + mechanical bowel preparation (OR 0.62 (95 per cent c.i. 0.41 to 0.94)) compared with intravenous antibiotics alone. There was no significant difference in outcomes with mechanical bowel preparation in the absence of intravenous antibiotics and oral antibiotics in the main analysis.
Conclusion: A bowel preparation strategy with intravenous antibiotics + oral antibiotics, with or without mechanical bowel preparation, should represent the standard of care for patients undergoing elective colorectal surgery.
© The Author(s) 2023. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
Comment in
-
Mechanical and oral antibiotic bowel preparation for all patients undergoing colorectal surgery?BJS Open. 2023 May 5;7(3):zrad048. doi: 10.1093/bjsopen/zrad048. BJS Open. 2023. PMID: 37257058 Free PMC article. No abstract available.
References
-
- Young H, Knepper B, Moore EE, Johnson JL, Mehler P, Price CS. Surgical site infection after colon surgery: national healthcare safety network risk factors and modeled rates compared with published risk factors and rates. J Am Coll Surg 2012;214:852–859 - PubMed
-
- Biondo S, Kreisler E, Fraccalvieri D, Basany EE, Codina-Cazador A, Ortiz H. Risk factors for surgical site infection after elective resection for rectal cancer. A multivariate analysis on 2131 patients. Colorectal Dis 2012;14:e95–e102 - PubMed
-
- Kingham TP, Pachter HL. Colonic anastomotic leak: risk factors, diagnosis, and treatment. J Am Coll Surg 2009;208:269–278 - PubMed
-
- Park JS, Choi GS, Kim SH, Kim HR, Kim NK, Lee KYet al. . Multicenter analysis of risk factors for anastomotic leakage after laparoscopic rectal cancer excision: the Korean laparoscopic colorectal surgery study group. Ann Surg 2013;257:665–671 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
