

Children's Oncology Group AALL1331: Phase III Trial of Blinatumomab in Children, Adolescents, and Young Adults With Low-Risk B-Cell ALL in First Relapse
- PMID: 37257143
- PMCID: PMC10852366
- DOI: 10.1200/JCO.22.02200
Children's Oncology Group AALL1331: Phase III Trial of Blinatumomab in Children, Adolescents, and Young Adults With Low-Risk B-Cell ALL in First Relapse
Abstract
Purpose: Blinatumomab, a bispecific T-cell engager immunotherapy, is efficacious in relapsed/refractory B-cell ALL (B-ALL) and has a favorable toxicity profile. One aim of the Children's Oncology Group AALL1331 study was to compare survival of patients with low-risk (LR) first relapse of B-ALL treated with chemotherapy alone or chemotherapy plus blinatumomab.
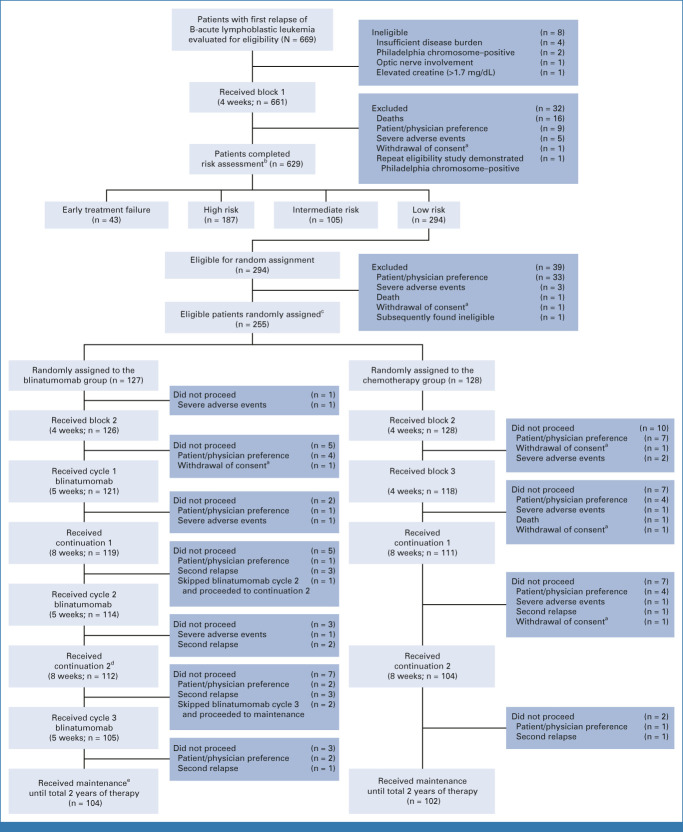
Patients and methods: After block 1 reinduction, patients age 1-30 years with LR first relapse of B-ALL were randomly assigned to block 2/block 3/two continuation chemotherapy cycles/maintenance (arm C) or block 2/two cycles of continuation chemotherapy intercalated with three blinatumomab blocks/maintenance (arm D). Patients with CNS leukemia received 18 Gy cranial radiation during maintenance and intensified intrathecal chemotherapy. The primary and secondary end points were disease-free survival (DFS) and overall survival (OS).
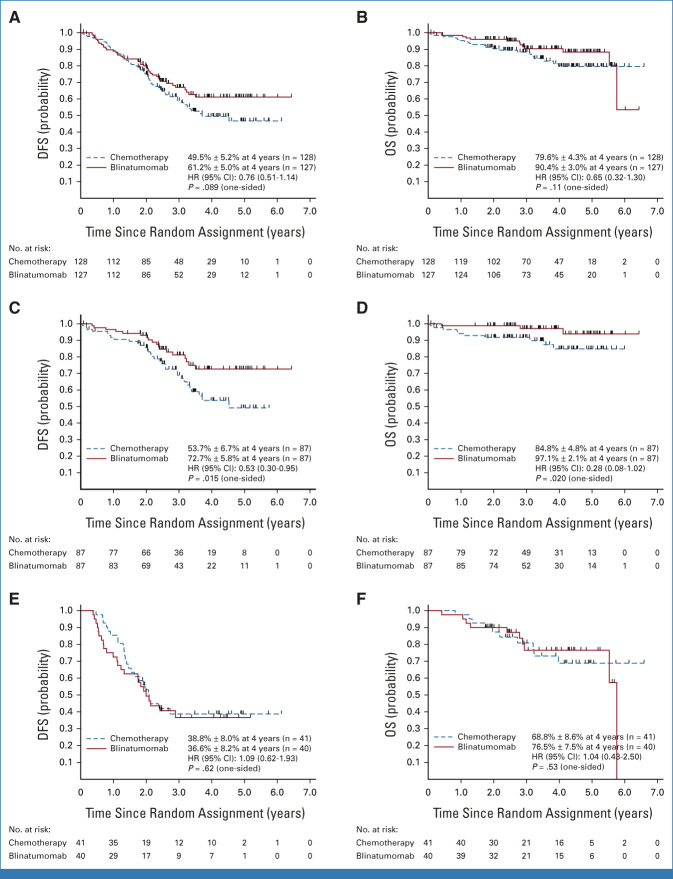
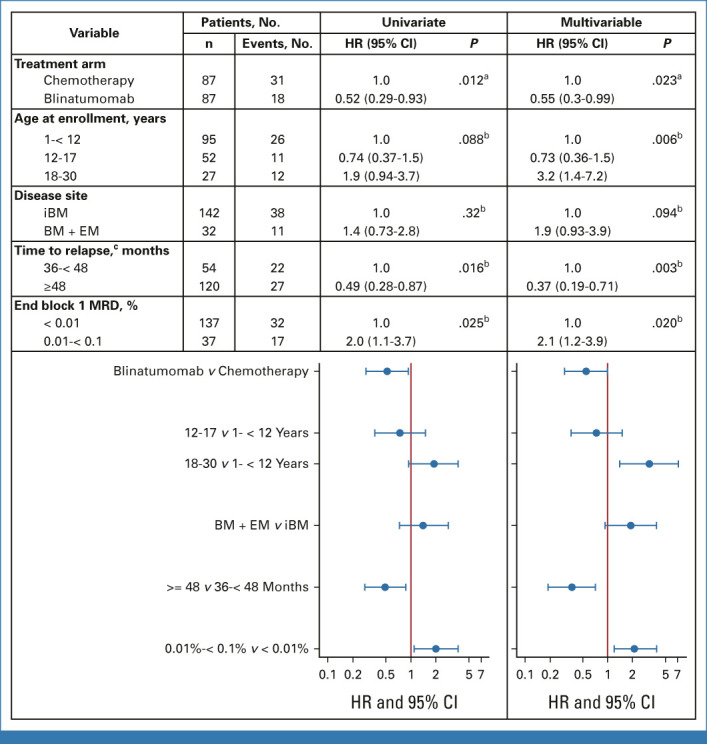
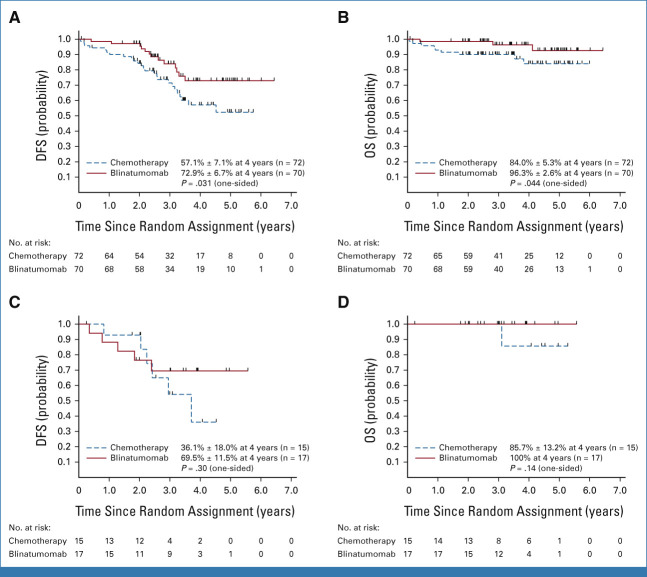
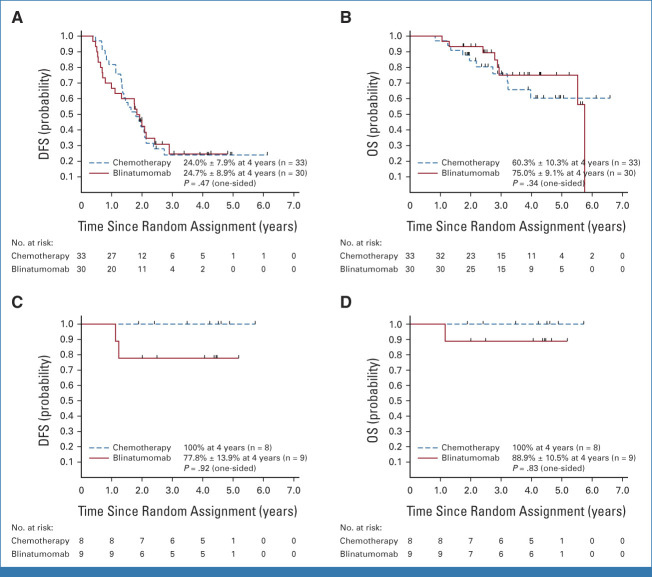
Results: The 4-year DFS/OS for the 255 LR patients accrued between December 2014 and September 2019 were 61.2% ± 5.0%/90.4% ± 3.0% for blinatumomab versus 49.5% ± 5.2%/79.6% ± 4.3% for chemotherapy (P = .089/P = .11). For bone marrow (BM) ± extramedullary (EM) (BM ± EM; n = 174) relapses, 4-year DFS/OS were 72.7% ± 5.8%/97.1% ± 2.1% for blinatumomab versus 53.7% ± 6.7%/84.8% ± 4.8% for chemotherapy (P = .015/P = .020). For isolated EM (IEM; n = 81) relapses, 4-year DFS/OS were 36.6% ± 8.2%/76.5% ± 7.5% for blinatumomab versus 38.8% ± 8.0%/68.8% ± 8.6% for chemotherapy (P = .62/P = .53). Blinatumomab was well tolerated and patients had low adverse event rates.
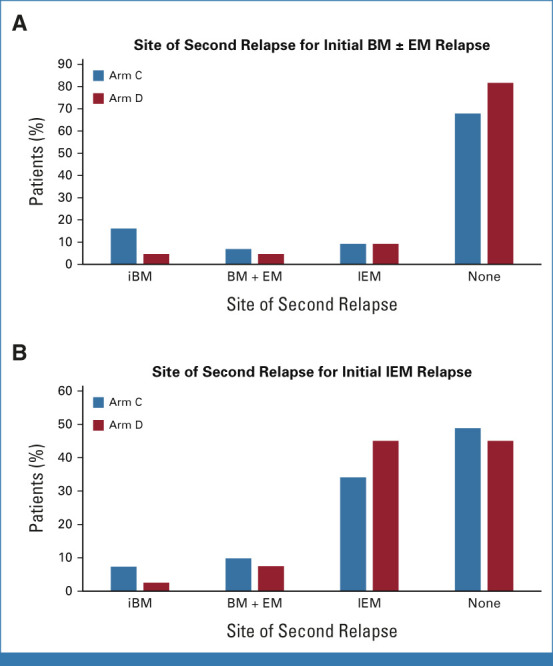
Conclusion: For children, adolescents, and young adults with B-ALL in LR first relapse, there was no statistically significant difference in DFS or OS between the blinatumomab and standard chemotherapy arms overall. However, blinatumomab significantly improved DFS and OS for the two thirds of patients with BM ± EM relapse, establishing a new standard of care for this population. By contrast, similar outcomes and poor DFS for both arms were observed in the one third of patients with IEM; new treatment approaches are needed for these patients (ClinicalTrials.gov identifier: NCT02101853).
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures
Comment in
-
Blinatumomab improves outcomes for pediatric patients with low-risk B-cell acute lymphoblastic leukemia in first marrow relapse.Transl Pediatr. 2024 Mar 27;13(3):530-534. doi: 10.21037/tp-23-521. Epub 2024 Mar 6. Transl Pediatr. 2024. PMID: 38590377 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
