

Multidisciplinary Critical Care Management of Electrical Storm: JACC State-of-the-Art Review
- PMID: 37257955
- PMCID: PMC10683004
- DOI: 10.1016/j.jacc.2023.03.424
Multidisciplinary Critical Care Management of Electrical Storm: JACC State-of-the-Art Review
Abstract
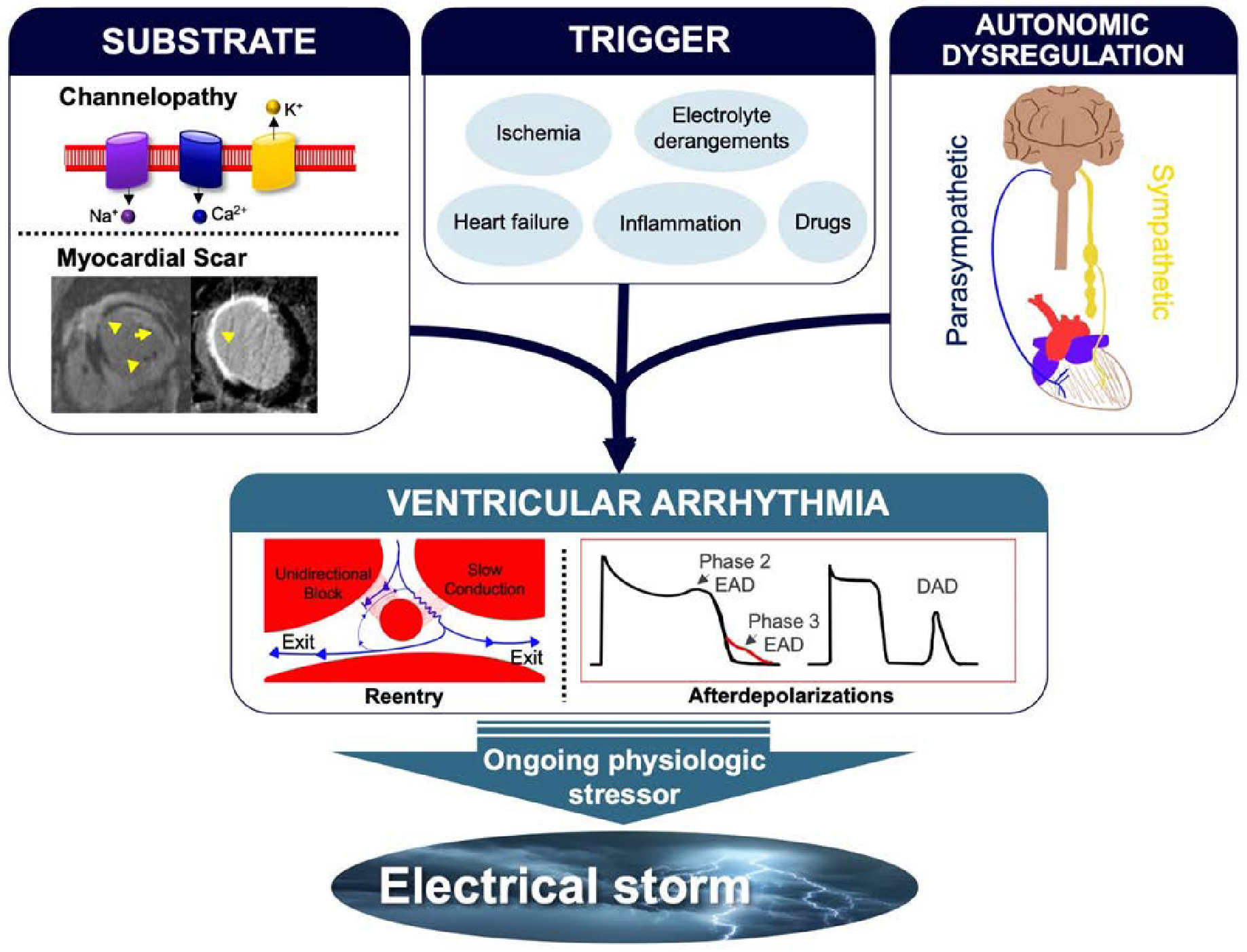
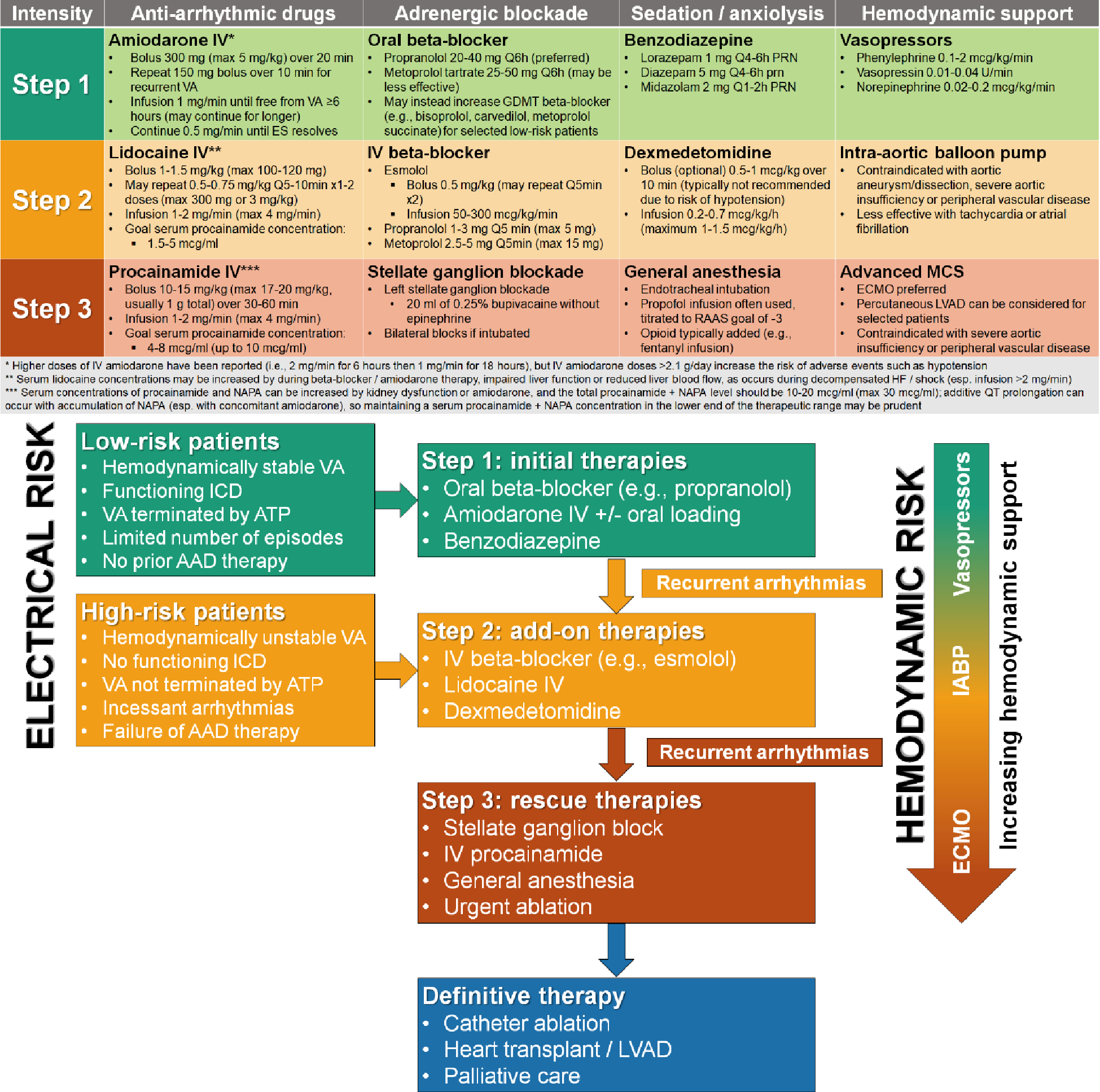
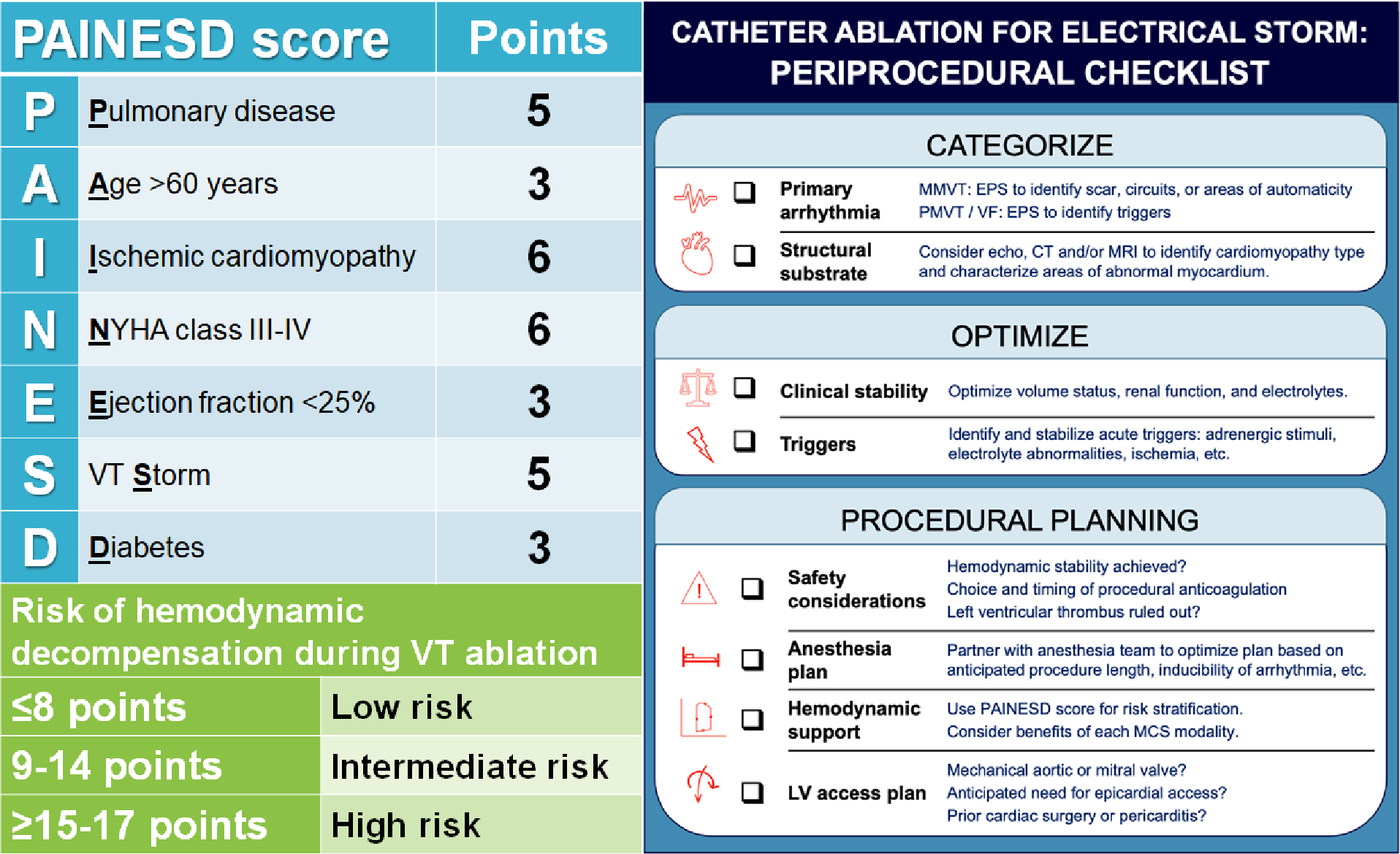
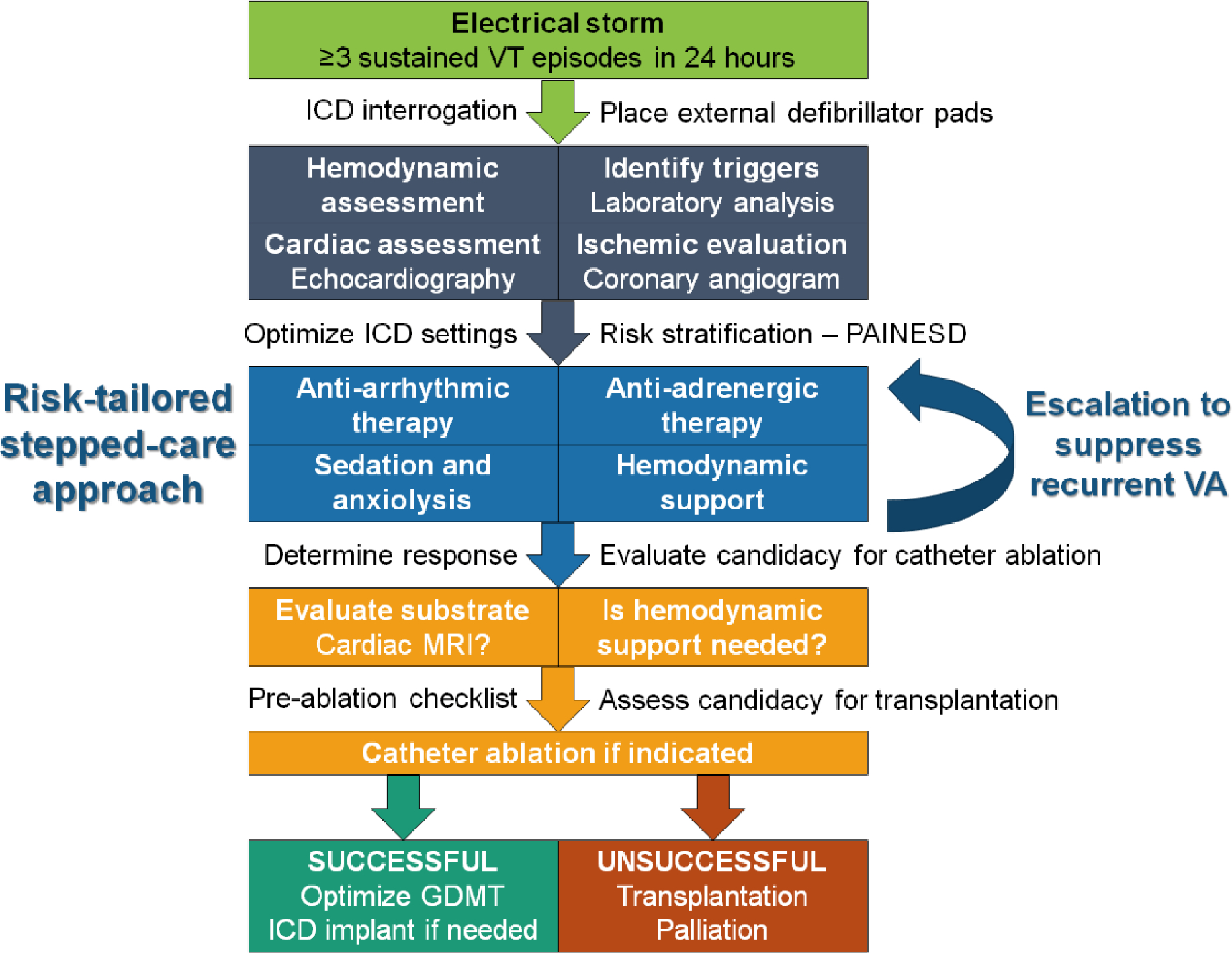
Electrical storm (ES) reflects life-threatening cardiac electrical instability with 3 or more ventricular arrhythmia episodes within 24 hours. Identification of underlying arrhythmogenic cardiac substrate and reversible triggers is essential, as is interrogation and programming of an implantable cardioverter-defibrillator, if present. Medical management includes antiarrhythmic drugs, beta-adrenergic blockade, sedation, and hemodynamic support. The initial intensity of these interventions should be matched to the severity of ES using a stepped-care algorithm involving escalating treatments for higher-risk presentations or recurrent ventricular arrhythmias. Many patients with ES are considered for catheter ablation, which may require the use of temporary mechanical circulatory support. Outcomes after ES are poor, including frequent ES recurrences and deaths caused by progressive heart failure and other cardiac causes. A multidisciplinary collaborative approach to the management of ES is crucial, and evaluation for heart transplantation or palliative care is often appropriate, even for patients who survive the initial episode.
Keywords: cardiomyopathy; heart failure; implantable cardioverter-defibrillator; myocardial infarction; shock; sudden cardiac death; ventricular fibrillation; ventricular tachycardia.
Copyright © 2023 American College of Cardiology Foundation. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures No extramural funding was directly involved in the conduct of this research. Dr Noseworthy has received research funding from National Institutes of Health (including the National Heart, Lung, and Blood Institute [R21AG 62580-1, R01HL 131535-4, R01HL 143070-2] and the National Institute on Aging [R01AG 062436-1]), Agency for Healthcare Research and Quality (R01HS 25402-3), U.S. Food and Drug Administration (FD 06292), and the American Heart Association (18SFRN34230146); he and Mayo Clinic have filed patents related to the application of artificial intelligence to electrocardiography for diagnosis and risk stratification and have licensed several artificial intelligence–electrocardiography algorithms to Anumana; he and Mayo Clinic are involved in potential equity/royalty relationship with AliveCor; he has served as a study investigator in an ablation trial sponsored by Medtronic; and has served on an expert advisory panel for OptumLabs. Dr Kashou is supported by the National Institutes of Health (T32 HL007111) and the Department of Cardiovascular Medicine at Mayo Clinic. Dr May has equity rights and possibly royalties received by the Mayo Clinic from Anumana Inc. Dr Chrispin has served on the Advisory Board for Biosense Webster; and has received honorarium from Abbott for educational activities. Dr Tisdale is supported by the National Heart, Lung, and Blood Institute, the American Heart Association, and the Indiana Clinical and Translational Sciences Institute. Dr Solomon is employed by the National Institutes of Health; and has received research support from the National Institutes of Health Clinical Center intramural research funds; this written work does not represent the official opinion of the U.S. government. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Al-Khatib SM, Stevenson WG, Ackerman MJ et al. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2018;72:e91–e220. - PubMed
-
- Zeppenfeld K, Tfelt-Hansen J, de Riva M et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022;43:3997–4126. - PubMed
-
- Bansch D, Bocker D, Brunn J, Weber M, Breithardt G, Block M. Clusters of ventricular tachycardias signify impaired survival in patients with idiopathic dilated cardiomyopathy and implantable cardioverter defibrillators. J Am Coll Cardiol 2000;36:566–73. - PubMed
-
- Exner DV, Pinski SL, Wyse DG et al. Electrical storm presages nonsudden death: the antiarrhythmics versus implantable defibrillators (AVID) trial. Circulation 2001;103:2066–71. - PubMed
-
- Arya A, Haghjoo M, Dehghani MR et al. Prevalence and predictors of electrical storm in patients with implantable cardioverter-defibrillator. Am J Cardiol 2006;97:389–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
