

Prognosis of immune checkpoint inhibitors-induced myocarditis: a case series
- PMID: 37258037
- PMCID: PMC10254993
- DOI: 10.1136/jitc-2022-004792
Prognosis of immune checkpoint inhibitors-induced myocarditis: a case series
Abstract
Background: Immune checkpoint inhibitors (ICI) have transformed cancer treatment over the last decade. Alongside this therapeutic improvement, a new variety of side effects has emerged, called immune-related adverse events (irAEs), potentially affecting any organ. Among these irAEs, myocarditis is rare but life-threatening.
Methods: We conducted a multicenter cross-sectional retrospective study with the aim of better characterizing ICI-related myocarditis. Myocarditis diagnosis was based on the recent consensus statement of the International Cardio-Oncology Society.
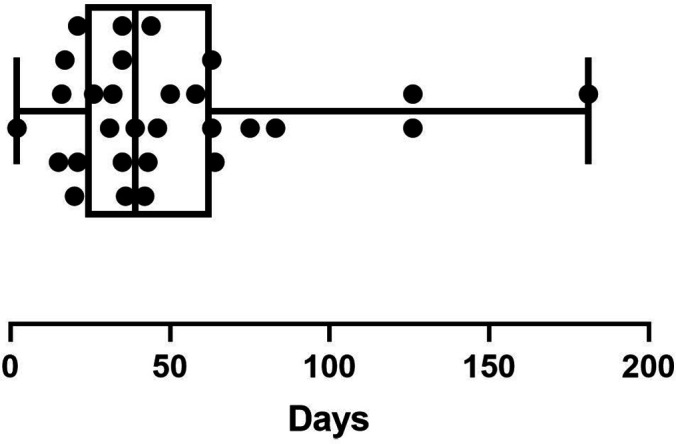
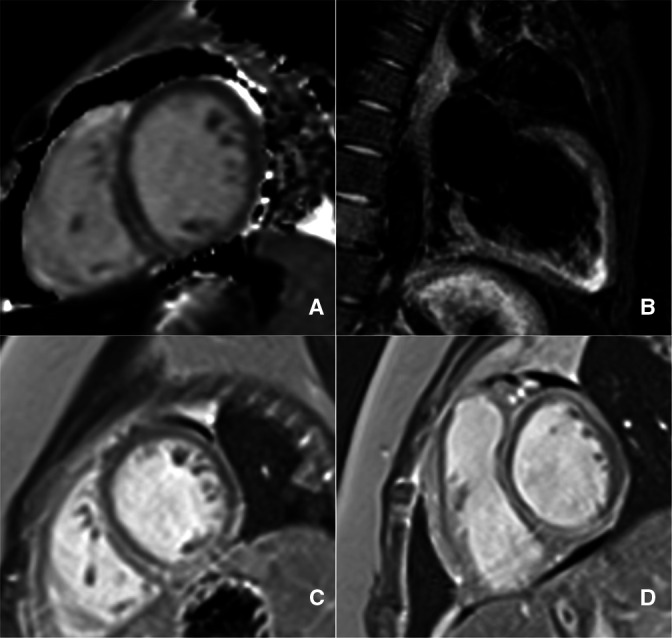
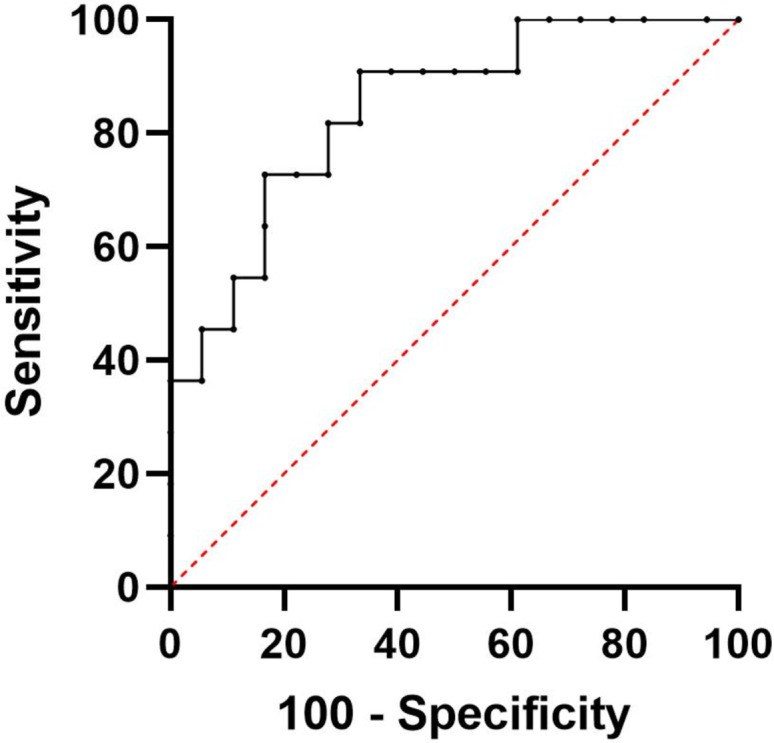
Results: Twenty-nine patients were identified, from six different referral centers. Most patients (55%) were treated using anti-programmed-death 1, rather than ICI combination (35%) or anti-programmed-death-ligand 1 (10%). Transthoracic echocardiography was abnormal in 52% of them, and cardiac magnetic resonance showed abnormal features in 14/24 patients (58%). Eleven patients (38%) were classified as severe. Compared with other patients, they had more frequently pre-existing systemic autoimmune disease (45% vs 6%, p=0.018), higher troponin level on admission (42-fold the upper limit vs 3.55-fold, p=0.001), and exhibited anti-acetylcholine receptor autoantibodies (p=0.001). Seven patients (24%) had myocarditis-related death, and eight more patients died from cancer progression during follow-up. Twenty-eight patients received glucocorticoids, 10 underwent plasma exchanges, 8 received intravenous immunoglobulins, and 5 other immunosuppressants. ICI rechallenge was performed in six patients, with only one myocarditis relapse.
Discussion: The management of ICI-related myocarditis may be challenging and requires a multidisciplinary approach. Prognostic features are herein described and may help to allow ICI rechallenge for some patients with smoldering presentation, after an accurate evaluation of benefit-risk balance.
Keywords: Immunotherapy; Lung Neoplasms; Melanoma; Programmed Cell Death 1 Receptor.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AM has received fees from AbbVie, Actelion, CSL Behring, Experf, Novartis, and Shire and declares speaking fees from AstraZeneca, Sanofi-Aventis and BMS in the last 5 years. PG is a medical expert for LFB (Laboratoire Français du Biofractionnement) and has received fees from AbbVie, Actelion, Boehringer Ingelheim France, Bouchara-Recordati, Novartis, Pfizer, and Roche in the last 5 years. Other authors declare that they have no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials