

Automated LVO detection and collateral scoring on CTA using a 3D self-configuring object detection network: a multi-center study
- PMID: 37258516
- PMCID: PMC10232534
- DOI: 10.1038/s41598-023-33723-w
Automated LVO detection and collateral scoring on CTA using a 3D self-configuring object detection network: a multi-center study
Abstract
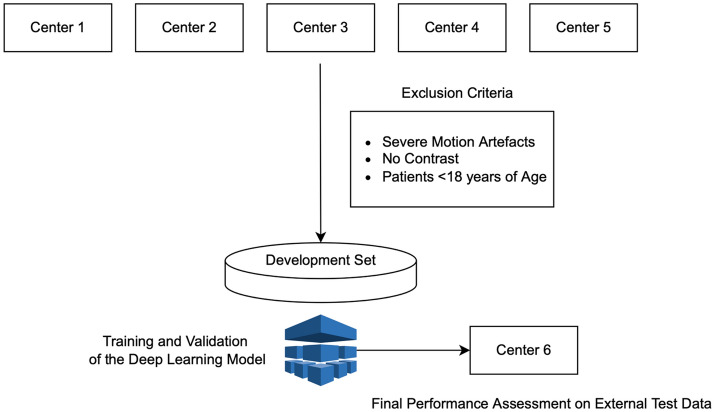
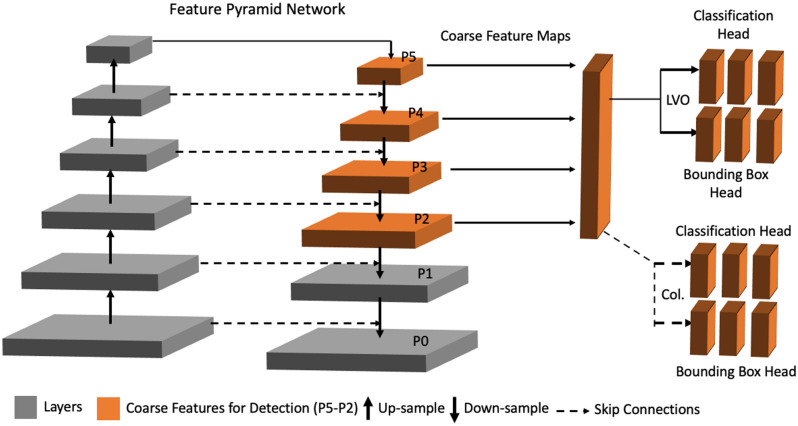
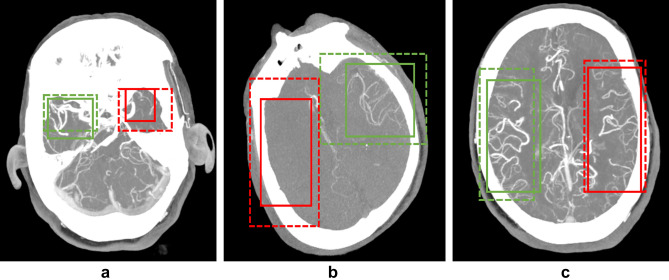
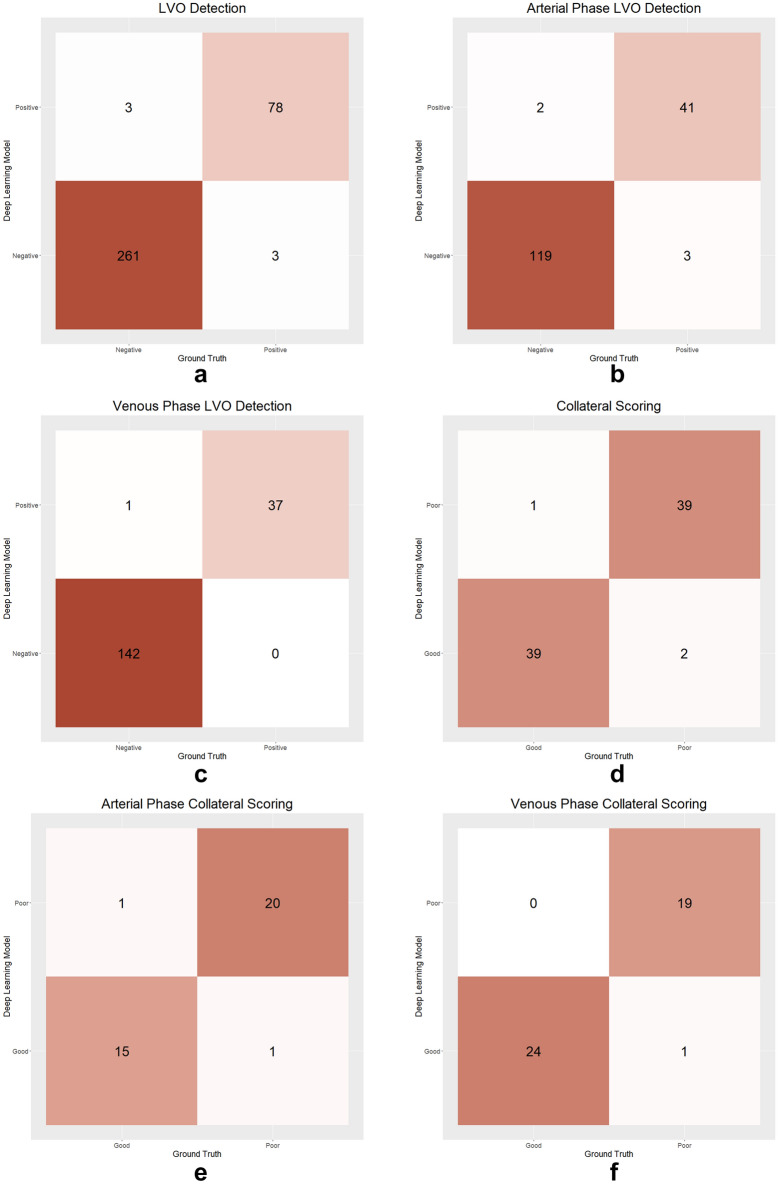
The use of deep learning (DL) techniques for automated diagnosis of large vessel occlusion (LVO) and collateral scoring on computed tomography angiography (CTA) is gaining attention. In this study, a state-of-the-art self-configuring object detection network called nnDetection was used to detect LVO and assess collateralization on CTA scans using a multi-task 3D object detection approach. The model was trained on single-phase CTA scans of 2425 patients at five centers, and its performance was evaluated on an external test set of 345 patients from another center. Ground-truth labels for the presence of LVO and collateral scores were provided by three radiologists. The nnDetection model achieved a diagnostic accuracy of 98.26% (95% CI 96.25-99.36%) in identifying LVO, correctly classifying 339 out of 345 CTA scans in the external test set. The DL-based collateral scores had a kappa of 0.80, indicating good agreement with the consensus of the radiologists. These results demonstrate that the self-configuring 3D nnDetection model can accurately detect LVO on single-phase CTA scans and provide semi-quantitative collateral scores, offering a comprehensive approach for automated stroke diagnostics in patients with LVO.
© 2023. The Author(s).
Conflict of interest statement
D.A. is the CEO and co-founder of Hevi AI Health Tech. M.Y. is the chief AI scientist and co-founder of Hevi AI Health Tech. Other authors declare no interest.
Figures

References
-
- WHO EMRO|Stroke, Cerebrovascular accident|Health topics. World Health Organization-Regional Office for the Eastern Mediterranean.http://www.emro.who.int/health-topics/stroke-cerebrovascular-accident/in....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
