

Multi-omic features of oesophageal adenocarcinoma in patients treated with preoperative neoadjuvant therapy
- PMID: 37258531
- PMCID: PMC10232490
- DOI: 10.1038/s41467-023-38891-x
Multi-omic features of oesophageal adenocarcinoma in patients treated with preoperative neoadjuvant therapy
Abstract
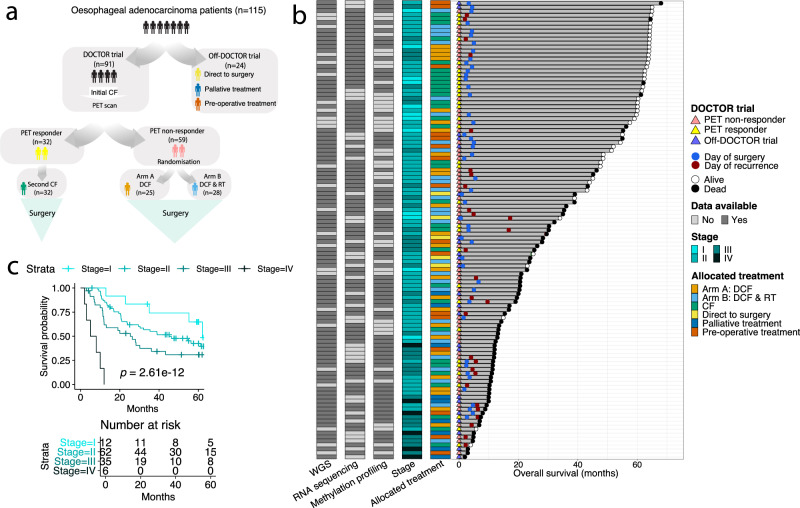
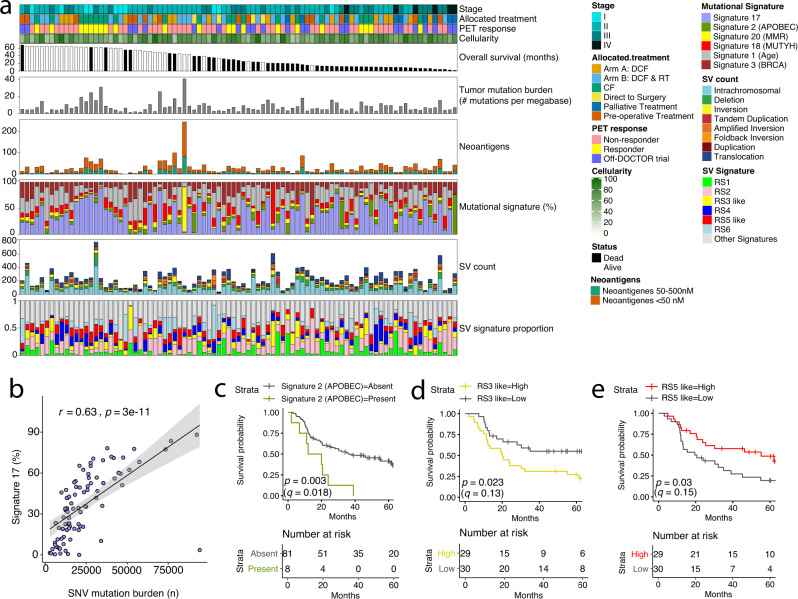
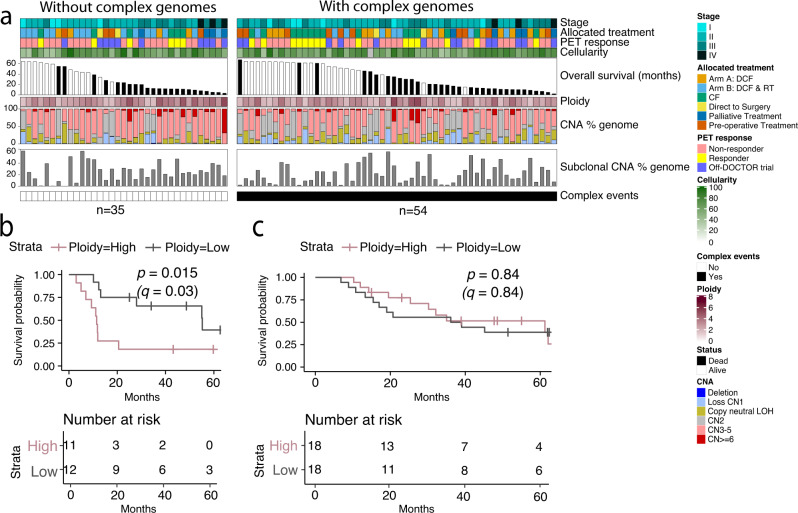
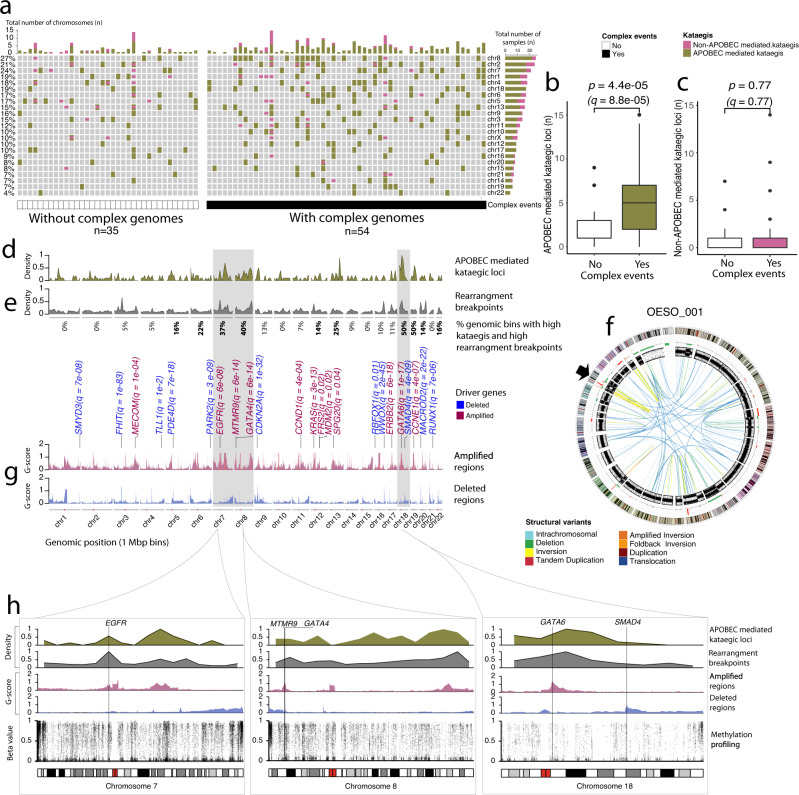
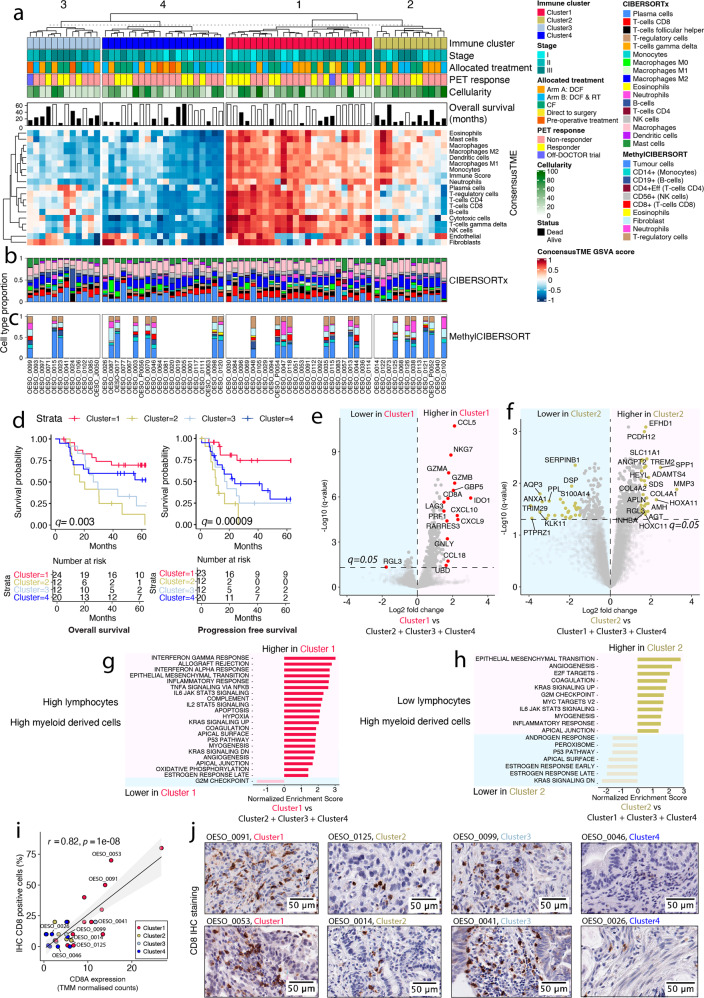
Oesophageal adenocarcinoma is a poor prognosis cancer and the molecular features underpinning response to treatment remain unclear. We investigate whole genome, transcriptomic and methylation data from 115 oesophageal adenocarcinoma patients mostly from the DOCTOR phase II clinical trial (Australian New Zealand Clinical Trials Registry-ACTRN12609000665235), with exploratory analysis pre-specified in the study protocol of the trial. We report genomic features associated with poorer overall survival, such as the APOBEC mutational and RS3-like rearrangement signatures. We also show that positron emission tomography non-responders have more sub-clonal genomic copy number alterations. Transcriptomic analysis categorises patients into four immune clusters correlated with survival. The immune suppressed cluster is associated with worse survival, enriched with myeloid-derived cells, and an epithelial-mesenchymal transition signature. The immune hot cluster is associated with better survival, enriched with lymphocytes, myeloid-derived cells, and an immune signature including CCL5, CD8A, and NKG7. The immune clusters highlight patients who may respond to immunotherapy and thus may guide future clinical trials.
© 2023. The Author(s).
Conflict of interest statement
J.V.P. and N.W. are founders of genomiQa Pty Ltd, and members of its Board. All other authors have no competing interests.
Figures

References
-
- Collaborators, G.B.D.O.C. The global, regional, and national burden of oesophageal cancer and its attributable risk factors in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020;5:582–597. doi: 10.1016/S2468-1253(20)30007-8. - DOI - PMC - PubMed
-
- Kato, K. et al. Pembrolizumab plus chemotherapy versus chemotherapy as first-line therapy in patients with advanced esophageal cancer: the phase 3 KEYNOTE-590 study. Ann. Oncol.31, S1192–S1193 (2020).
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
