

Optimising the yield from bronchoalveolar lavage on human participants in infectious disease immunology research
- PMID: 37258565
- PMCID: PMC10231287
- DOI: 10.1038/s41598-023-35723-2
Optimising the yield from bronchoalveolar lavage on human participants in infectious disease immunology research
Abstract
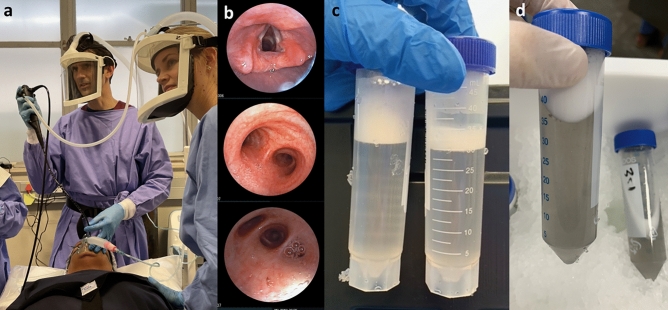
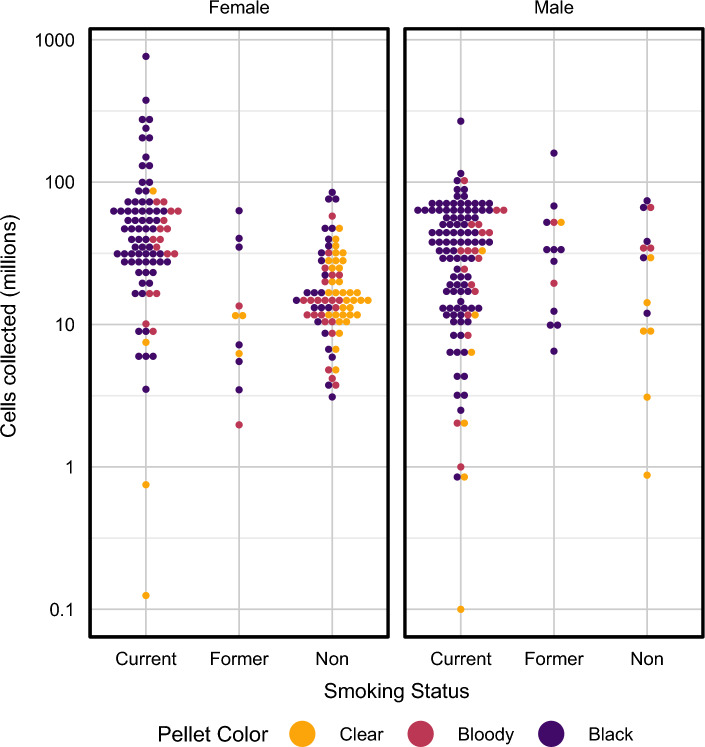
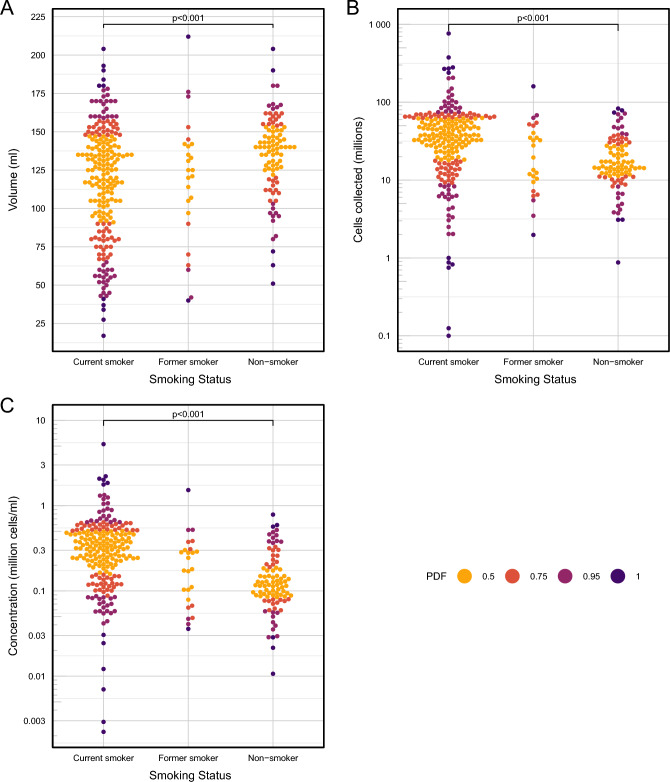
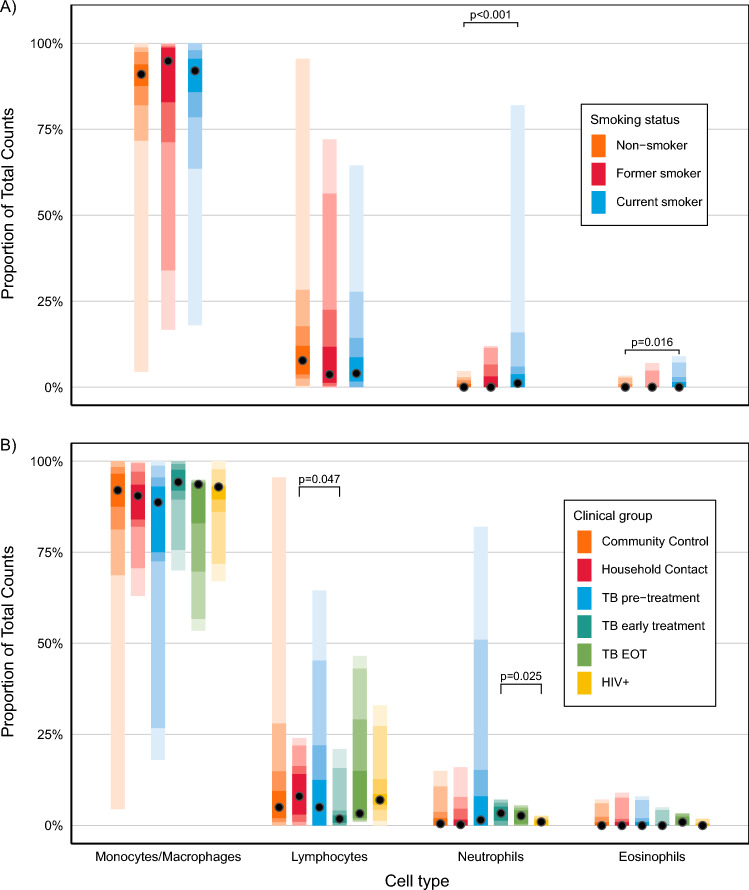
Bronchoalveolar lavage (BAL) is becoming a common procedure for research into infectious disease immunology. Little is known about the clinical factors which influence the main outcomes of the procedure. In research participants who underwent BAL according to guidelines, the BAL volume yield, and cell yield, concentration, viability, pellet colour and differential count were analysed for association with important participant characteristics such as active tuberculosis (TB) disease, TB exposure, HIV infection and recent SARS-CoV-2 infection. In 337 participants, BAL volume and BAL cell count were correlated in those with active TB disease, and current smokers. The right middle lobe yielded the highest volume. BAL cell and volume yields were lower in older participants, who also had more neutrophils. Current smokers yielded lower volumes and higher numbers of all cell types, and usually had a black pellet. Active TB disease was associated with higher cell yields, but this declined at the end of treatment. HIV infection was associated with more bloody pellets, and recent SARS-CoV-2 infection with a higher proportion of lymphocytes. These results allow researchers to optimise their participant and end assay selection for projects involving lung immune cells.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Update of
-
Optimising the yield from bronchoalveolar lavage on human participants in infectious disease immunology research.Res Sq [Preprint]. 2023 Feb 2:rs.3.rs-2505850. doi: 10.21203/rs.3.rs-2505850/v1. Res Sq. 2023. Update in: Sci Rep. 2023 May 31;13(1):8859. doi: 10.1038/s41598-023-35723-2. PMID: 36778283 Free PMC article. Updated. Preprint.
References
-
- Du Rand, I. A. et al. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: accredited by NICE. Thorax68, i1 LP-i44 (2013). - PubMed
-
- Löfdahl, J. M., Cederlund, K., Nathell, L., Eklund, A. & Sköld, C. M. Bronchoalveolar lavage in COPD: fluid recovery correlates with the degree of emphysema. Eur. Respir. J.25, 275 LP–281 (2005). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
