

Exercise Capacity and Ventilatory Efficiency in Patients With Pulmonary Arterial Hypertension
- PMID: 37260024
- PMCID: PMC10382004
- DOI: 10.1161/JAHA.122.026890
Exercise Capacity and Ventilatory Efficiency in Patients With Pulmonary Arterial Hypertension
Abstract
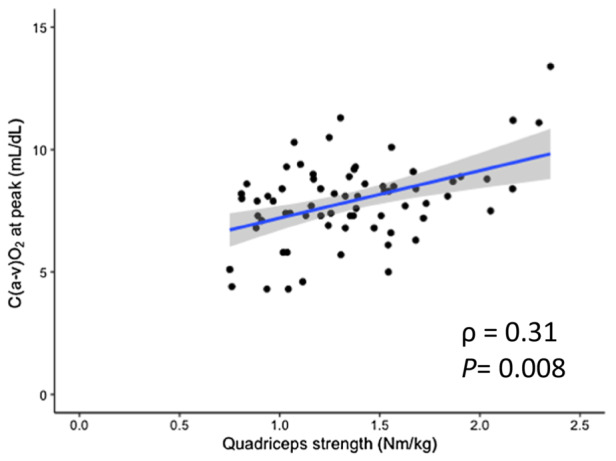
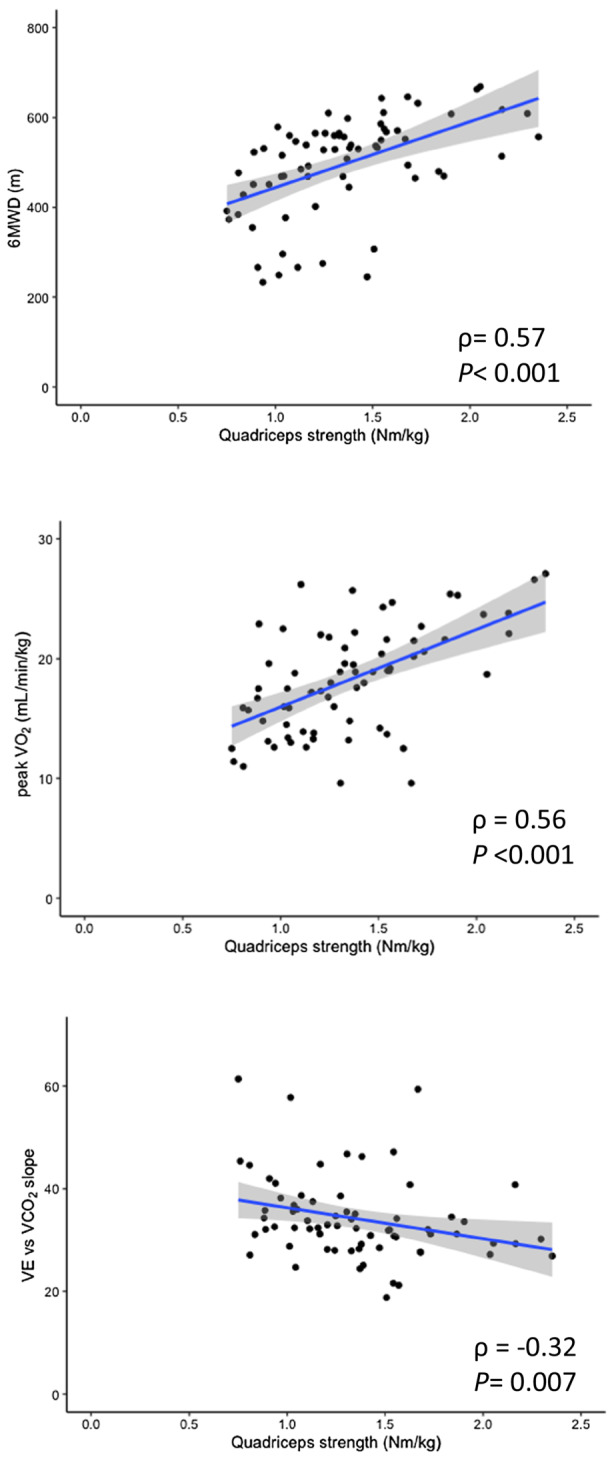
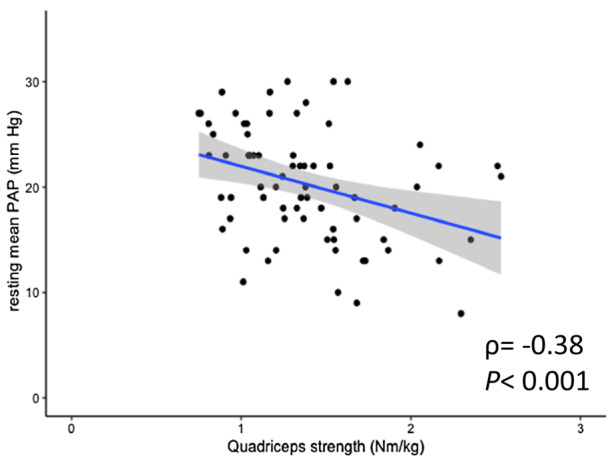
Background The symptom for identification of pulmonary arterial hypertension (PAH) is dyspnea on exertion, with a concomitant decrease in exercise capacity. Even patients with hemodynamically improved PAH may have impaired exercise tolerance; however, the effect of central and peripheral factors on exercise tolerance remains unclear. We explored the factors contributing to exercise capacity and ventilatory efficiency in patients with hemodynamically normalized PAH after medical treatment. Methods and Results In total, 82 patients with PAH (age: median 46 [interquartile range, 39-51] years; male:female, 23:59) and mean pulmonary arterial pressure ≤30 mm Hg at rest were enrolled. The exercise capacity, indicated by the 6-minute walk distance and peak oxygen consumption, and the ventilatory efficiency, indicated by the minute ventilation versus carbon dioxide output slope, were assessed using cardiopulmonary exercise testing with a right heart catheter. The mean pulmonary arterial pressure was 21 (17-25) mm Hg, and the 6-minute walk distance was 530 (458-565) m, whereas the peak oxygen consumption was 18.8 (14.8-21.6) mLꞏmin-1ꞏkg-1. The multivariate model that best predicted 6-minute walk distance included peak arterial mixed venous oxygen content difference (β=0.46, P<0.001), whereas the best peak oxygen consumption predictors included peak cardiac output (β=0.72, P<0.001), peak arterial mixed venous oxygen content difference (β=0.56, P<0.001), and resting mean pulmonary arterial pressure (β=-0.25, P=0.026). The parameter that best predicted minute ventilation versus carbon dioxide output slope was the resting mean pulmonary arterial pressure (β=0.35, P=0.041). Quadriceps muscle strength was moderately correlated with exercise capacity (6-minute walk distance; ρ=0.57, P<0.001; peak oxygen consumption: ρ=0.56, P<0.001) and weakly correlated with ventilatory efficiency (ρ=-0.32, P=0.007). Conclusions Central and peripheral factors are closely related to impaired exercise tolerance in patients with hemodynamically normalized PAH.
Keywords: 6‐minute walk distance; exercise capacity; hemodynamics; muscle strength; pulmonary arterial hypertension; ventilatory efficiency.
Figures
References
-
- Humbert M, Guignabert C, Bonnet S, Dorfmüller P, Klinger JR, Nicolls MR, Olschewski AJ, Pullamsetti SS, Schermuly RT, Stenmark KR, et al. Pathology and pathobiology of pulmonary hypertension: state of the art and research perspectives. Eur Respir J. 2019;53:53. doi: 10.1183/13993003.01887-2018 - DOI - PMC - PubMed
-
- Tobita K, Goda A, Nishida Y, Takeuchi K, Kikuchi H, Inami T, Kohno T, Yamada S, Soejima K, Satoh T. Factors contributing to exercise capacity in chronic thromboembolic pulmonary hypertension with near‐normal hemodynamics. J Heart Lung Transplant. 2021;40:677–686. doi: 10.1016/j.healun.2021.03.003 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
