

Lung cancer risk discrimination of prediagnostic proteomics measurements compared with existing prediction tools
- PMID: 37260165
- PMCID: PMC10483263
- DOI: 10.1093/jnci/djad071
Lung cancer risk discrimination of prediagnostic proteomics measurements compared with existing prediction tools
Abstract
Background: We sought to develop a proteomics-based risk model for lung cancer and evaluate its risk-discriminatory performance in comparison with a smoking-based risk model (PLCOm2012) and a commercially available autoantibody biomarker test.
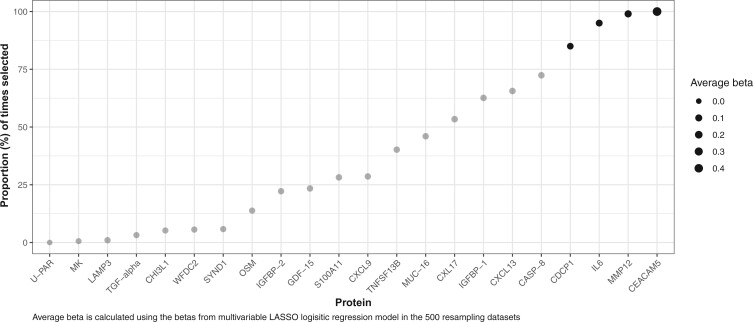
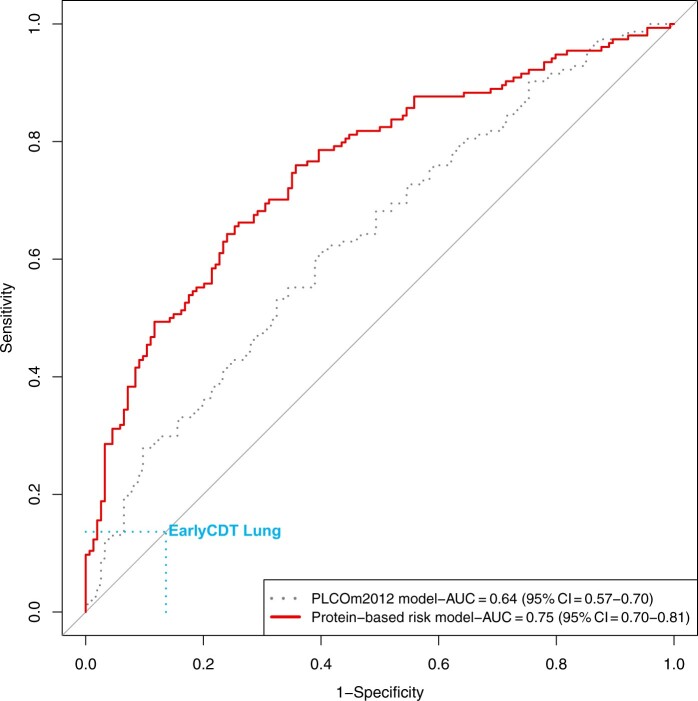
Methods: We designed a case-control study nested in 6 prospective cohorts, including 624 lung cancer participants who donated blood samples at most 3 years prior to lung cancer diagnosis and 624 smoking-matched cancer free participants who were assayed for 302 proteins. We used 470 case-control pairs from 4 cohorts to select proteins and train a protein-based risk model. We subsequently used 154 case-control pairs from 2 cohorts to compare the risk-discriminatory performance of the protein-based model with that of the Early Cancer Detection Test (EarlyCDT)-Lung and the PLCOm2012 model using receiver operating characteristics analysis and by estimating models' sensitivity. All tests were 2-sided.
Results: The area under the curve for the protein-based risk model in the validation sample was 0.75 (95% confidence interval [CI] = 0.70 to 0.81) compared with 0.64 (95% CI = 0.57 to 0.70) for the PLCOm2012 model (Pdifference = .001). The EarlyCDT-Lung had a sensitivity of 14% (95% CI = 8.2% to 19%) and a specificity of 86% (95% CI = 81% to 92%) for incident lung cancer. At the same specificity of 86%, the sensitivity for the protein-based risk model was estimated at 49% (95% CI = 41% to 57%) and 30% (95% CI = 23% to 37%) for the PLCOm2012 model.
Conclusion: Circulating proteins showed promise in predicting incident lung cancer and outperformed a standard risk prediction model and the commercialized EarlyCDT-Lung.
© The Author(s) 2023. Published by Oxford University Press.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, et al.Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249. - PubMed
-
- Paci E, Puliti D, Lopes Pegna A, et al.; for the ITALUNG Working Group. Mortality, survival and incidence rates in the ITALUNG randomised lung cancer screening trial. Thorax. 2017;72(9):825-831. - PubMed
-
- Rota M, Pizzato M, La Vecchia C, et al.Efficacy of lung cancer screening appears to increase with prolonged intervention: results from the MILD trial and a meta-analysis. Ann Oncol. 2019;30(7):1040-1043. - PubMed
-
- Becker N, Motsch E, Trotter A, et al.Lung cancer mortality reduction by LDCT screening-results from the randomized German LUSI trial. Int J Cancer. 2020;146(6):1503-1513. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 CA144034/CA/NCI NIH HHS/United States
- 1000143/MRC_/Medical Research Council/United Kingdom
- MR/M012190/1/MRC_/Medical Research Council/United Kingdom
- R01 CA080205/CA/NCI NIH HHS/United States
- 001/WHO_/World Health Organization/International
- C18281/A29019/CRUK_/Cancer Research UK/United Kingdom
- 29017/CRUK_/Cancer Research UK/United Kingdom
- C8221/A29017/CRUK_/Cancer Research UK/United Kingdom
- 14136/CRUK_/Cancer Research UK/United Kingdom
- U19 CA203654/CA/NCI NIH HHS/United States
- R03 CA245979/CA/NCI NIH HHS/United States
- R01 CA262164/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
