

Sodium-glucose cotransporter-2 inhibitor therapy in kidney transplant patients with type 2 or post-transplant diabetes: an observational multicentre study
- PMID: 37260993
- PMCID: PMC10229265
- DOI: 10.1093/ckj/sfad007
Sodium-glucose cotransporter-2 inhibitor therapy in kidney transplant patients with type 2 or post-transplant diabetes: an observational multicentre study
Abstract
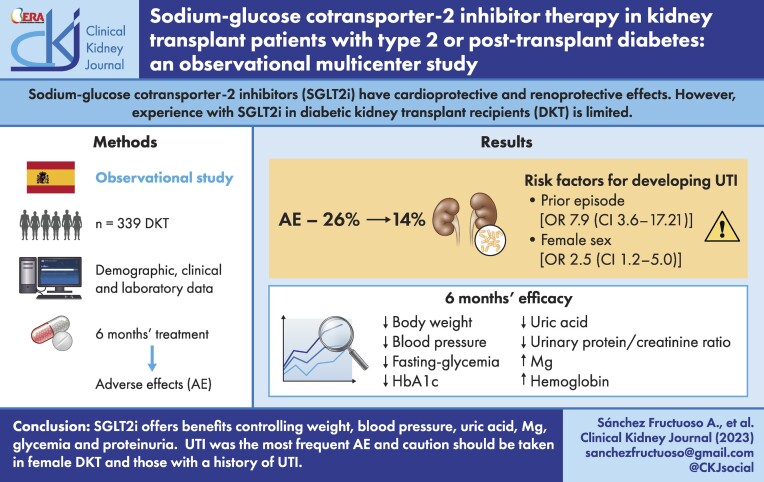
Background: Sodium-glucose cotransporter-2 inhibitors (SGLT2is) have cardioprotective and renoprotective effects. However, experience with SGLT2is in diabetic kidney transplant recipients (DKTRs) is limited.
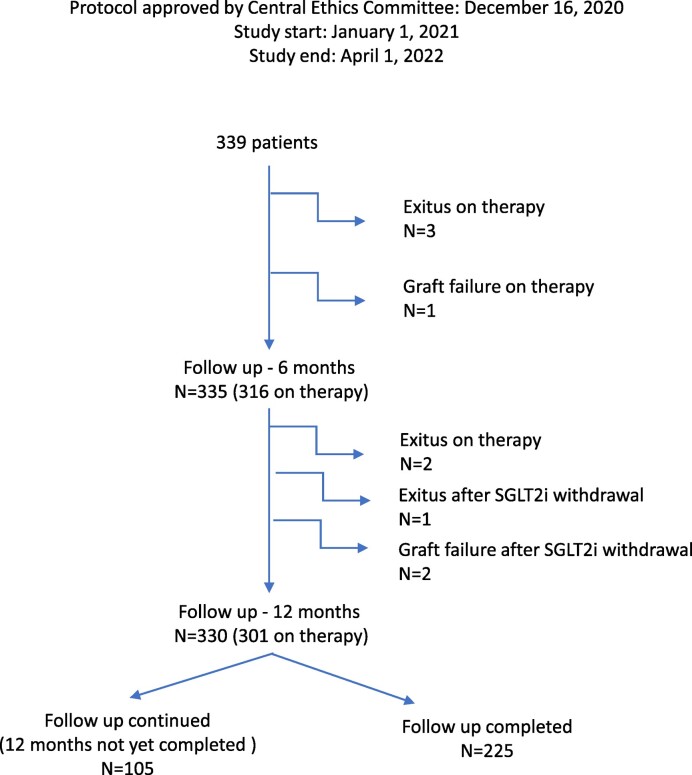
Methods: This observational multicentre study was designed to examine the efficacy and safety of SGLT2is in DKTRs. The primary outcome was adverse effects within 6 months of SGLT2i treatment.
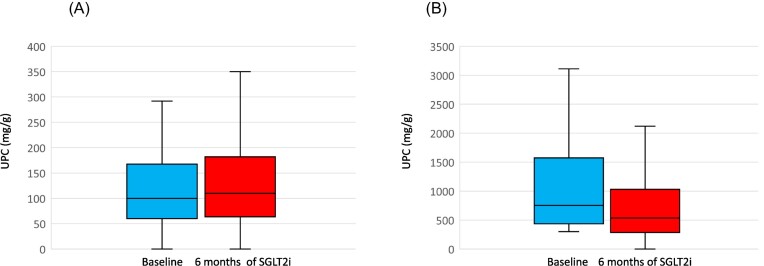
Results: Among 339 treated DKTRs, adverse effects were recorded in 26%, the most frequent (14%) being urinary tract infection (UTI). In 10%, SGLT2is were suspended mostly because of UTI. Risk factors for developing a UTI were a prior episode of UTI in the 6 months leading up to SGLT2i use {odds ratio [OR] 7.90 [confidence interval (CI) 3.63-17.21]} and female sex [OR 2.46 (CI 1.19-5.03)]. In a post hoc subgroup analysis, the incidence of UTI emerged as similar in DKTRs treated with SGLT2i for 12 months versus non-DKTRs (17.9% versus 16.7%). Between baseline and 6 months, significant reductions were observed in body weight [-2.22 kg (95% CI -2.79 to -1.65)], blood pressure, fasting glycaemia, haemoglobin A1c [-0.36% (95% CI -0.51 to -0.21)], serum uric acid [-0.44 mg/dl (95% CI -0.60 to -0.28)] and urinary protein:creatinine ratio, while serum magnesium [+0.15 mg/dl (95% CI 0.11-0.18)] and haemoglobin levels rose [+0.44 g/dl (95% CI 0.28-0.58]. These outcomes persisted in participants followed over 12 months of treatment.
Conclusions: SGLT2is in kidney transplant offer benefits in terms of controlling glycaemia, weight, blood pressure, anaemia, proteinuria and serum uric acid and magnesium. UTI was the most frequent adverse effect. According to our findings, these agents should be prescribed with caution in female DKTRs and those with a history of UTI.
Keywords: SGLT2 inhibitors; post-transplant diabetes mellitus; type 2 diabetes.
© The Author(s) 2023. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
None declared.
Figures
References
-
- Lim WH, Wong G, Pilmore HLet al. . Long-term outcomes of kidney transplantation in people with type 2 diabetes: a population cohort study. Lancet Diabetes Endocrinol 2017;5:26–33. - PubMed
-
- Hart A, Lentine KL, Smith JMet al. . OPTN/SRTR 2019 annual data report: kidney. Am J Transplant 2021;21:21–137. - PubMed
LinkOut - more resources
Full Text Sources
