

Paediatric pineal region cysts: enigma or impaired neurofluid system?
- PMID: 37261536
- PMCID: PMC10684616
- DOI: 10.1007/s00381-023-06000-4
Paediatric pineal region cysts: enigma or impaired neurofluid system?
Abstract
Purpose: Pineal region cysts (PCs) may affect the tectum and aqueduct and cause deep central vein congestion. Beside headaches, PC often causes a broad range of symptoms, leading to prolonged diagnosis and therapy. The aims of this study are to reveal parameters that might explain the ambiguity of the symptoms and to identify factors in association with the respiration-driven neurofluid system.
Methods: This retrospective study included 28 paediatric patients (mean age 11.6 years) who received surgical treatment and 18 patients (mean age 11.3 years) who were followed conservatively. Symptoms, time to diagnosis, cyst size, ventricular indices, head circumference and postoperative outcome, were analysed. Four patients were investigated for CSF dynamics with real-time MRI. The mean follow-up time was 1.6 years.
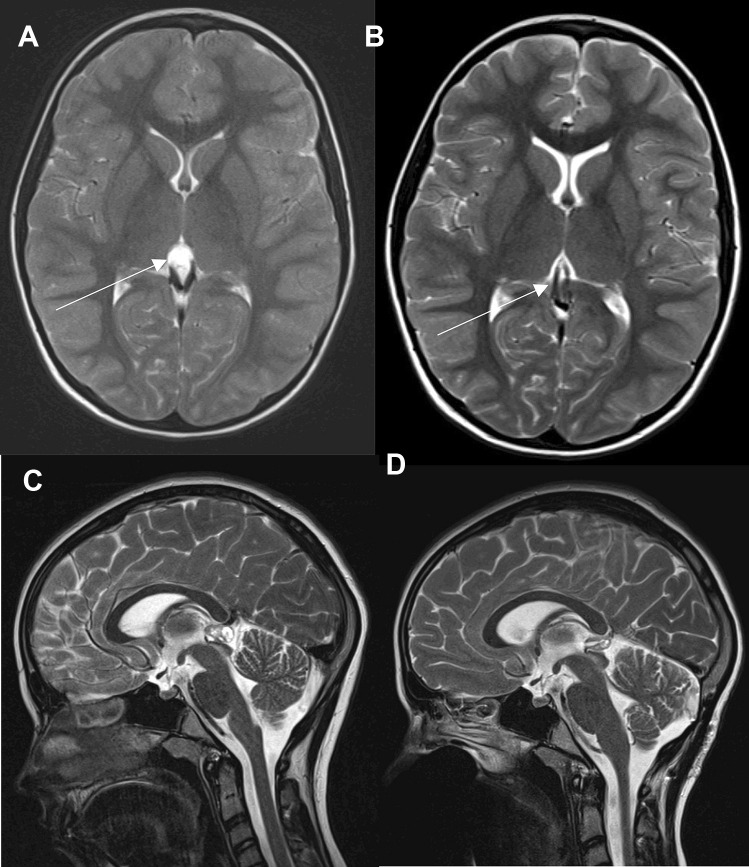
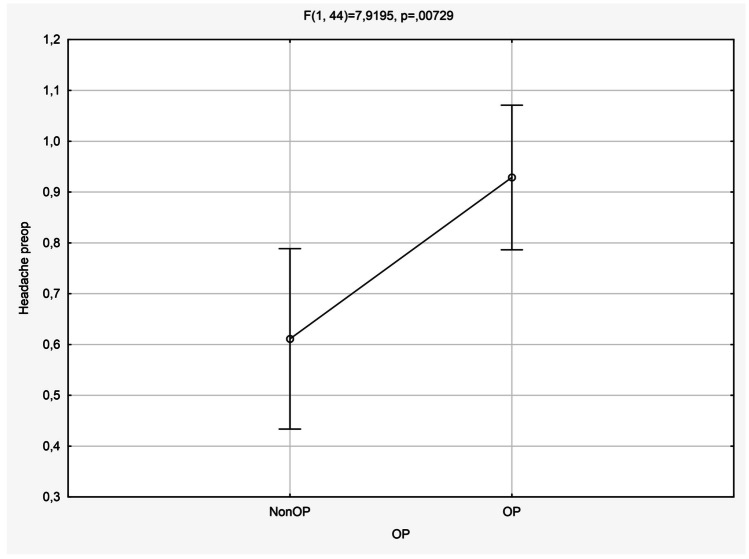
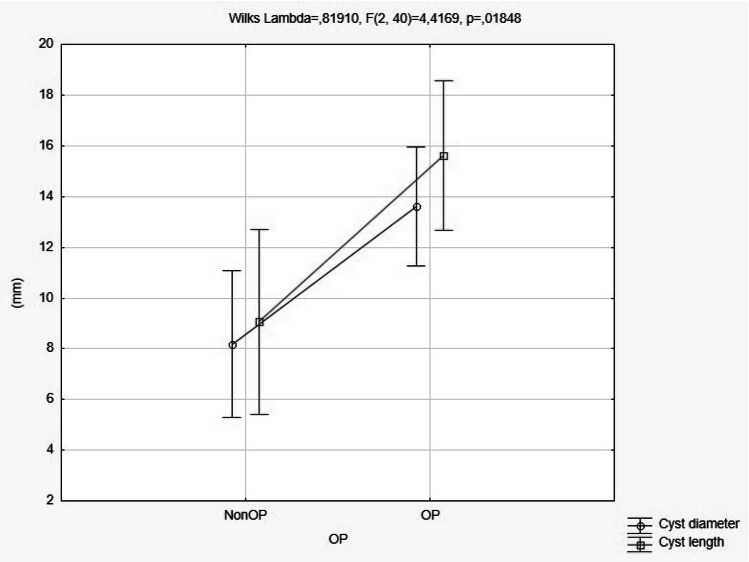
Results: The most common early onset symptoms were headaches (92%), blurred vision (42.8%), sleep disturbances (39.3%) and vertigo (32.1%). Tectum contact was observed in 82% of patients, and MRI examinations revealed that imaging flow void signals were absent in 32.1% of patients. The maximal cyst diameters were 13.7 × 15.6 mm (mean). Together with a postoperative flow void signal, 4 patients recovered their respiration-driven CSF aqueductal upward flow, which was not detectable preoperatively. After surgery the main symptoms improved.
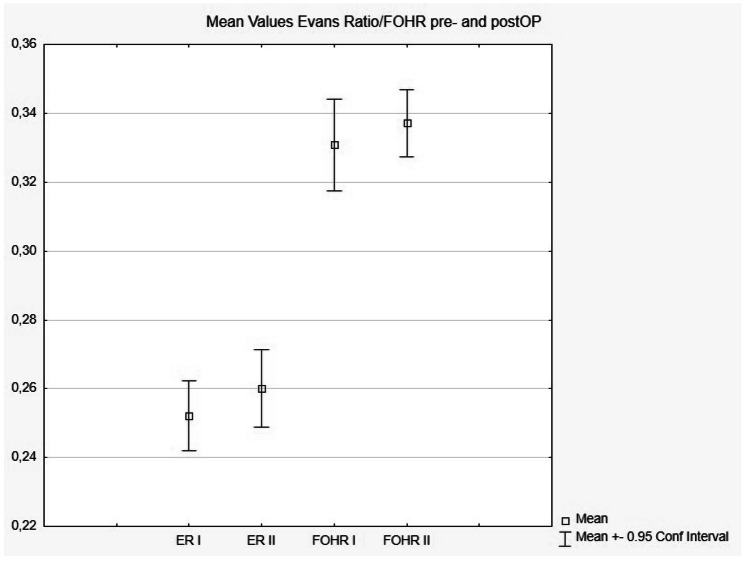
Conclusion: Despite proximity to the aqueduct with frequently absent flow void signals, hydrocephalus was never detected. Data from real-time MRI depicted a reduced preoperative filling of the ventricular CSF compartments, indicating a diminished fluid preload, which recovered postoperatively.
Keywords: Glymphatic system; Hydrocephalus; Microsurgery; Pineal cyst; Real-time MRI; Respiration.
© 2023. The Author(s).
Conflict of interest statement
None.
Figures

References
-
- Michielsen G, Benoit Y, Baert E et al (2002) Symptomatic pineal cysts: clinical manifestations and management. Acta neurochirurgica 144:233–42-discussion 242. 10.1007/s007010200031 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
