

Estradiol and Spironolactone Plasma Pharmacokinetics Among Brazilian Transgender Women Using HIV Pre-Exposure Prophylaxis: Analysis of Potential Interactions
- PMID: 37261664
- PMCID: PMC10338392
- DOI: 10.1007/s40262-023-01248-0
Estradiol and Spironolactone Plasma Pharmacokinetics Among Brazilian Transgender Women Using HIV Pre-Exposure Prophylaxis: Analysis of Potential Interactions
Abstract
Background and objective: An important barrier to HIV prevention among transgender women (TGW) is the concern that oral pre-exposure prophylaxis (PrEP) negatively affects the efficacy of feminizing hormone therapy (FHT). We aimed to assess the impact of PrEP on FHT pharmacokinetics (PK) among TGW from Brazil.
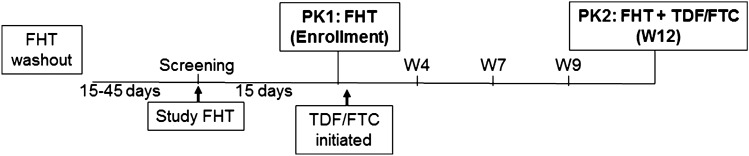
Methods: We performed a drug-drug interaction sub-study among TGW enrolled in a daily oral PrEP demonstration study (PrEParadas, NCT03220152). Participants had a first PK assessment (PK1) 15 days after FHT (estradiol valerate 2-6 mg plus spironolactone 100-200 mg) initiation and then started PrEP (tenofovir disoproxil fumarate 300 mg/emtricitabine 200 mg). A second PK evaluation was performed 12 weeks later (PK2). Blood samples were collected prior and after the directly observed dosing (0, 0.5, 1, 2, 4, 6, 8, and 24 hours). Pharmacokinetic parameters of estradiol, spironolactone, and metabolites were estimated by non-compartmental analysis (Monolix 2021R2, Lixoft®) and compared as geometric mean ratios (GMRs, 90% confidence interval [CI]).
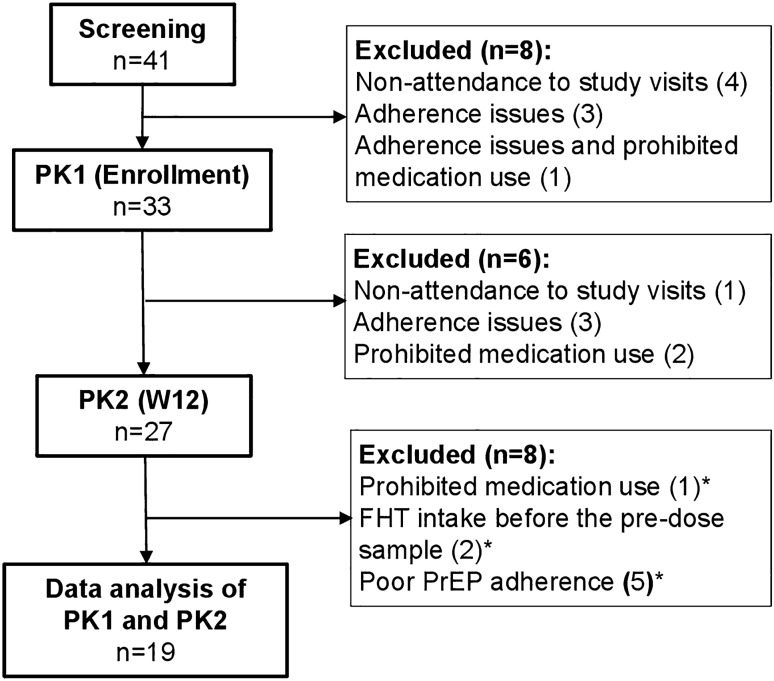
Results: Among 19 TGW who completed the substudy, median age was 26 years (interquartile range: 23-27.5). Estradiol area under the plasma concentration-time curve (AUCτ) and trough concentrations did not differ between PK1 and PK2 evaluations (GMR [90% CI]: 0.89 [0.76-1.04] and 1.06 [0.94-1.20], respectively). Spironolactone and canrenone AUCτ were statistically lower at PK2 than PK1 (0.76 [0.65-0.89] and 0.85 [0.78-0.94], respectively). Canrenone maximum concentration was also lower at PK2 than PK1 (0.82 [0.74-0.91]).
Conclusion: Estradiol PK was not influenced by PrEP concomitant use. The small differences observed in some spironolactone and canrenone PK parameters should not prevent the concomitant use of estradiol-based FHT and PrEP.
Trial registration: This trial (NCT03220152) was registered on July 18, 2017.
© 2023. The Author(s).
Conflict of interest statement
Peter Anderson has received consulting fees from Gilead, Merck, and ViiV, and research funding paid to his institution from Gilead. All other authors declare no competing interests.
Figures


References
-
- Ministerio da Saude. Secretaria de Vigilancia em Saude. Protocolo Clínico e Diretrizes Terapêuticas para Profilaxia Pré-Exposição (PrEP) de risco à infecção pelo HIV. Nov 23 2018. http://www.aids.gov.br/system/tdf/pub/2016/64510/miolo_pcdt_prep_11_2018.... Accessed 25 Nov 2018.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
