

Efficacy and Safety of 0.01% and 0.02% Atropine for the Treatment of Pediatric Myopia Progression Over 3 Years: A Randomized Clinical Trial
- PMID: 37261839
- PMCID: PMC10236322
- DOI: 10.1001/jamaophthalmol.2023.2097
Efficacy and Safety of 0.01% and 0.02% Atropine for the Treatment of Pediatric Myopia Progression Over 3 Years: A Randomized Clinical Trial
Erratum in
-
Clarifications for Primary and Secondary Outcomes and Analyses.JAMA Ophthalmol. 2023 Oct 1;141(10):1005. doi: 10.1001/jamaophthalmol.2023.4206. JAMA Ophthalmol. 2023. PMID: 37707831 Free PMC article. No abstract available.
Abstract
Importance: The global prevalence of myopia is predicted to approach 50% by 2050, increasing the risk of visual impairment later in life. No pharmacologic therapy is approved for treating childhood myopia progression.
Objective: To assess the safety and efficacy of NVK002 (Vyluma), a novel, preservative-free, 0.01% and 0.02% low-dose atropine formulation for treating myopia progression.
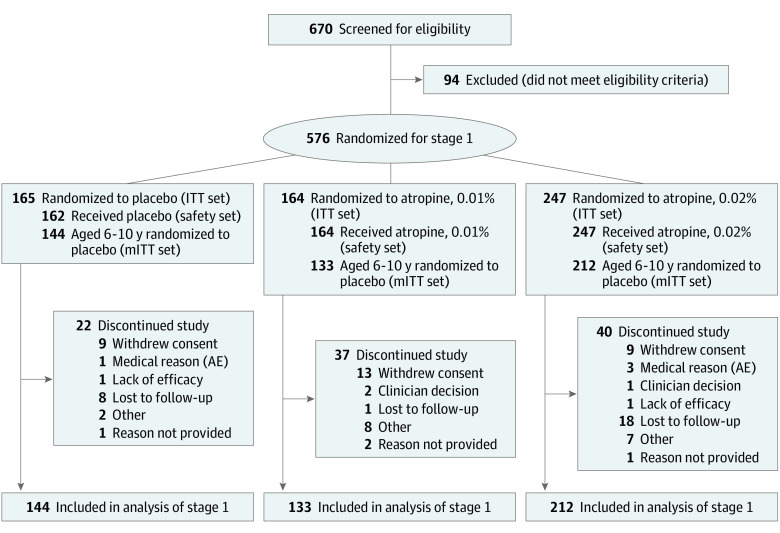
Design, setting, and participants: This was a double-masked, placebo-controlled, parallel-group, randomized phase 3 clinical trial conducted from November 20, 2017, through August 22, 2022, of placebo vs low-dose atropine, 0.01% and 0.02% (2:2:3 ratio). Participants were recruited from 26 clinical sites in North America and 5 countries in Europe. Enrolled participants were 3 to 16 years of age with -0.50 diopter (D) to -6.00 D spherical equivalent refractive error (SER) and no worse than -1.50 D astigmatism.
Interventions: Once-daily placebo, low-dose atropine, 0.01%, or low-dose atropine, 0.02%, eye drops for 36 months.
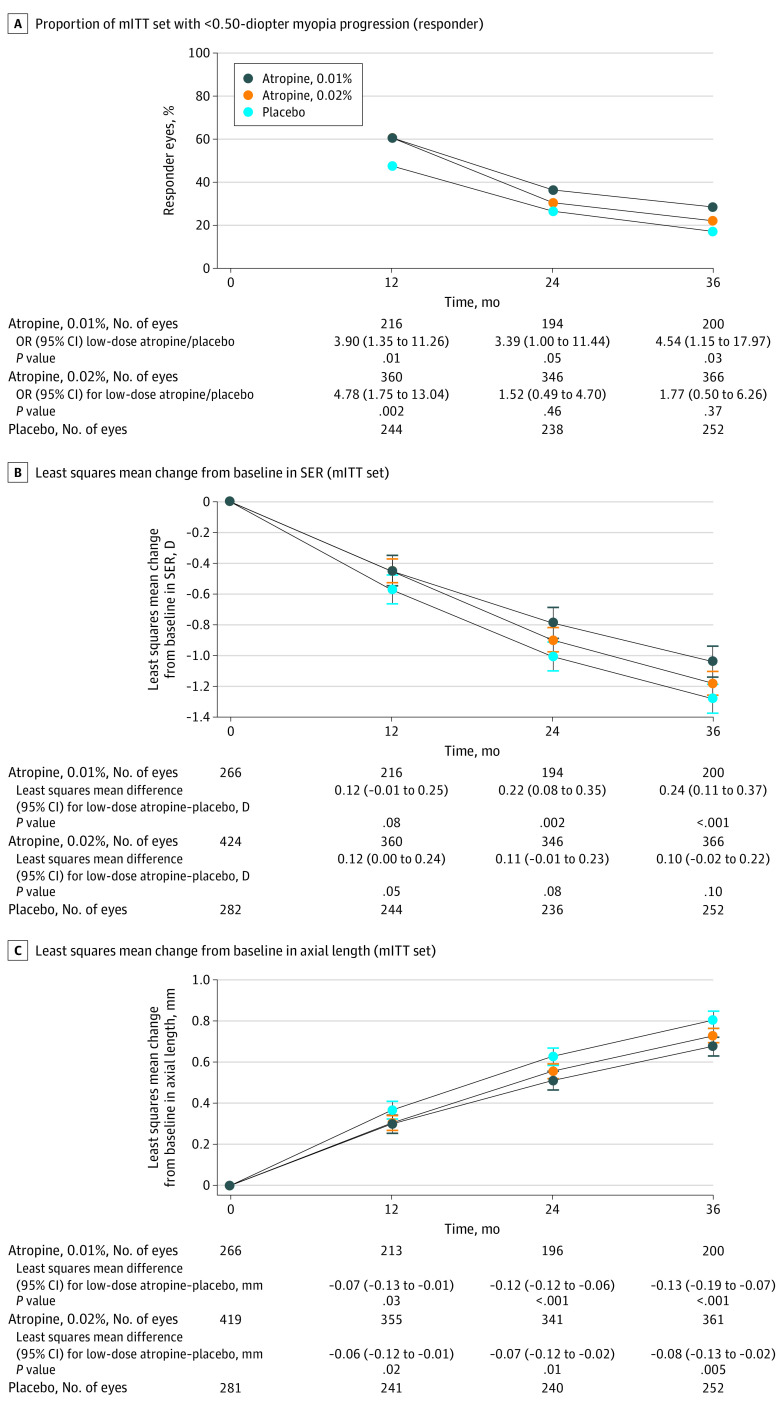
Main outcomes and measures: The primary, prespecified end point was the proportion of participants' eyes responding to 0.02% atropine vs placebo therapy (<0.50 D myopia progression at 36 months [responder analysis]). Secondary efficacy end points included responder analysis for atropine, 0.01%, and mean change from baseline in SER and axial length at month 36 in a modified intention-to-treat population (mITT; participants 6-10 years of age at baseline). Safety measurements for treated participants (3-16 years of age) were reported.
Results: A total of 576 participants were randomly assigned to treatment groups. Of these, 573 participants (99.5%; mean [SD] age, 8.9 [2.0] years; 315 female [54.7%]) received trial treatment (3 participants who were randomized did not receive trial drug) and were included in the safety set. The 489 participants (84.9%) who were 6 to 10 years of age at randomization composed the mITT set. At month 36, compared with placebo, low-dose atropine, 0.02%, did not significantly increase the responder proportion (odds ratio [OR], 1.77; 95% CI, 0.50-6.26; P = .37) or slow mean SER progression (least squares mean [LSM] difference, 0.10 D; 95% CI, -0.02 D to 0.22 D; P = .10) but did slow mean axial elongation (LSM difference, -0.08 mm; 95% CI, -0.13 mm to -0.02 mm; P = .005); however, at month 36, compared with placebo, low-dose atropine, 0.01%, significantly increased the responder proportion (OR, 4.54; 95% CI, 1.15-17.97; P = .03), slowed mean SER progression (LSM difference, 0.24 D; 95% CI, 0.11 D-0.37 D; P < .001), and slowed axial elongation (LSM difference, -0.13 mm; 95% CI, -0.19 mm to -0.07 mm; P < .001). There were no serious ocular adverse events and few serious nonocular events; none was judged as associated with atropine.
Conclusions and relevance: This randomized clinical trial found that 0.02% atropine did not significantly increase the proportion of participants' eyes responding to therapy but suggested efficacy for 0.01% atropine across all 3 main end points compared with placebo. The efficacy and safety observed suggest that low-dose atropine may provide a treatment option for childhood myopia progression.
Trial registration: ClinicalTrials.gov Identifier: NCT03350620.
Conflict of interest statement
Figures
Comment in
-
Is Recommending 0.01% Atropine for Myopia Control Clinically Meaningful?JAMA Ophthalmol. 2024 Mar 1;142(3):271-272. doi: 10.1001/jamaophthalmol.2023.6771. JAMA Ophthalmol. 2024. PMID: 38358758 No abstract available.
References
-
- Fricke TR, Jong M, Naidoo KS, et al. . Global prevalence of visual impairment associated with myopic macular degeneration and temporal trends from 2000 through 2050: systematic review, meta-analysis and modeling. Br J Ophthalmol. 2018;102(7):855-862. doi:10.1136/bjophthalmol-2017-311266 - DOI - PMC - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
