

Deep computational image analysis of immune cell niches reveals treatment-specific outcome associations in lung cancer
- PMID: 37264091
- PMCID: PMC10235089
- DOI: 10.1038/s41698-023-00403-x
Deep computational image analysis of immune cell niches reveals treatment-specific outcome associations in lung cancer
Abstract
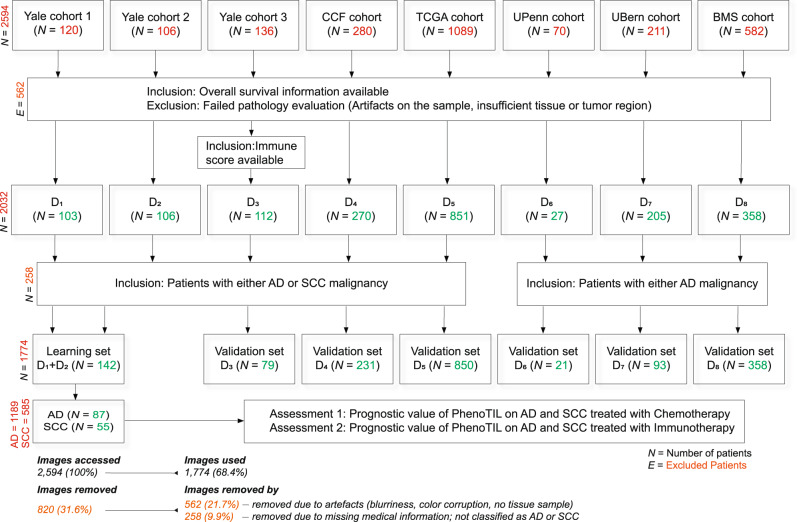
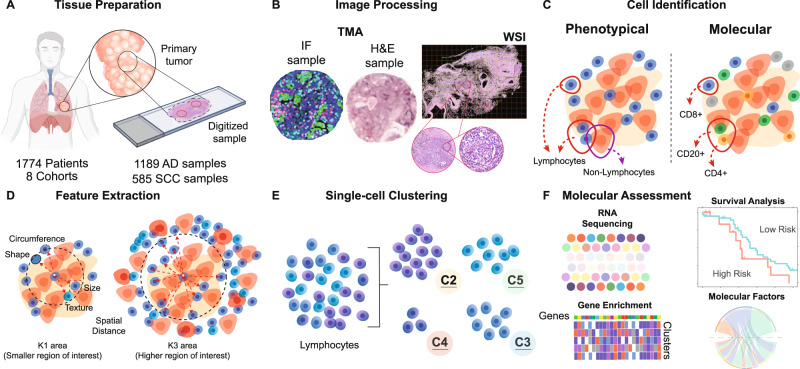
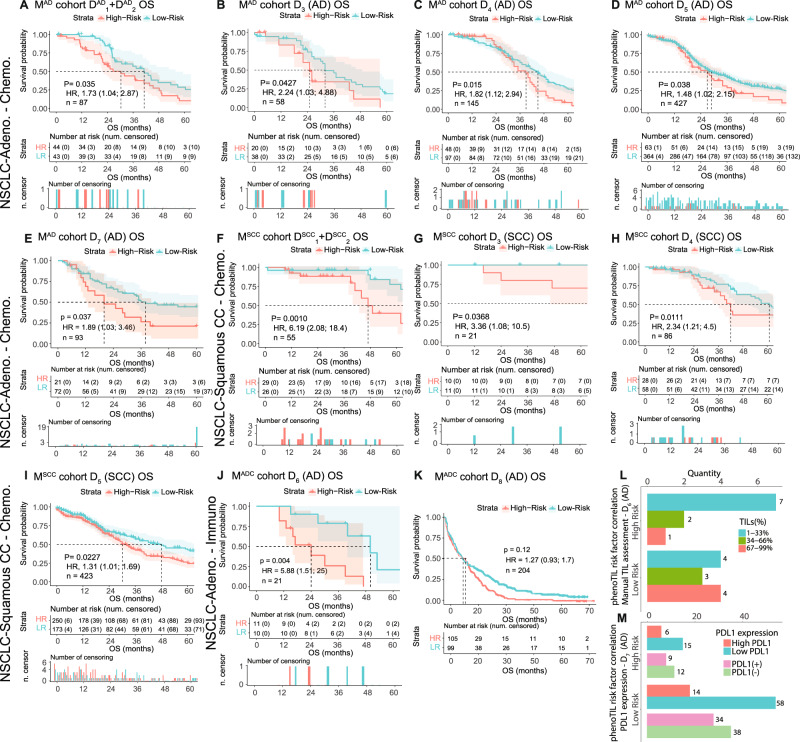
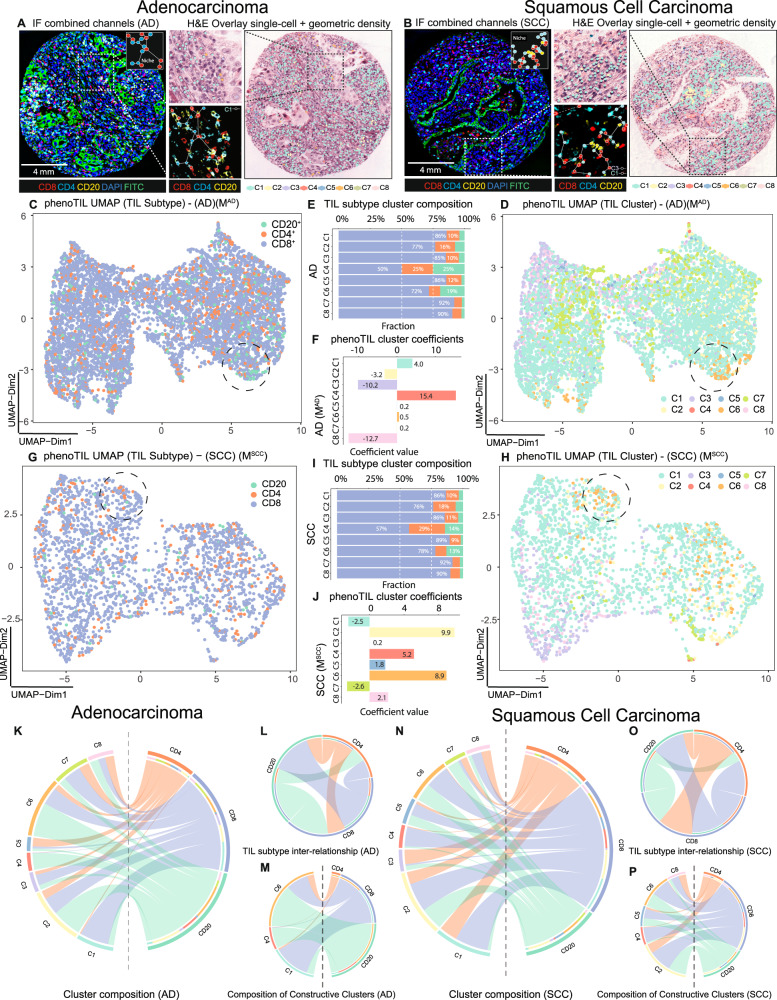
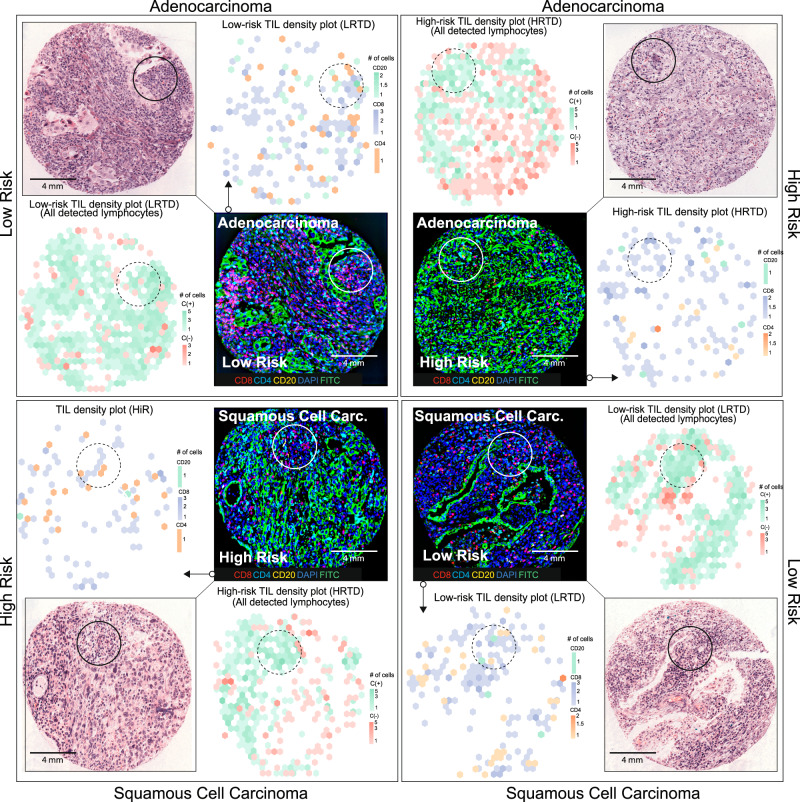
The tumor immune composition influences prognosis and treatment sensitivity in lung cancer. The presence of effective adaptive immune responses is associated with increased clinical benefit after immune checkpoint blockers. Conversely, immunotherapy resistance can occur as a consequence of local T-cell exhaustion/dysfunction and upregulation of immunosuppressive signals and regulatory cells. Consequently, merely measuring the amount of tumor-infiltrating lymphocytes (TILs) may not accurately reflect the complexity of tumor-immune interactions and T-cell functional states and may not be valuable as a treatment-specific biomarker. In this work, we investigate an immune-related biomarker (PhenoTIL) and its value in associating with treatment-specific outcomes in non-small cell lung cancer (NSCLC). PhenoTIL is a novel computational pathology approach that uses machine learning to capture spatial interplay and infer functional features of immune cell niches associated with tumor rejection and patient outcomes. PhenoTIL's advantage is the computational characterization of the tumor immune microenvironment extracted from H&E-stained preparations. Association with clinical outcome and major non-small cell lung cancer (NSCLC) histology variants was studied in baseline tumor specimens from 1,774 lung cancer patients treated with immunotherapy and/or chemotherapy, including the clinical trial Checkmate 057 (NCT01673867).
© 2023. The Author(s).
Conflict of interest statement
A.M. is an equity holder in Elucid Bioimaging, Picture Health and in Inspirata Inc. He is also a scientific advisory consultant for Aiforia Inc, Picture Health and SimbioSys. In addition, he has served as a scientific advisory board member for Inspirata Inc, Astrazeneca, Bristol-Myers-Squibb and Merck. He also has sponsored research agreements with Philips, Astrazeneca, Bristol-Myers Squibb, Boehringer-Ingelheim and Eli-Lilly. His technology has been licensed to Elucid Bioimaging and Picture Health. He also consults for Castle Biosciences, Biohme Inc. and SimbioSys. He is also involved in a NIH (National Institutes of Health) U24 grant with PathCore Inc, and 3 different R01 grants with Inspirata Inc. Kurt Schalper received research funding from Genoptix/Navigate (Novartis), Tesaro, Moderna Therapeutics, Takeda, Surface Oncology, Pierre-Fabre Research Institute, Merck, Bristol-Myers Squibb, AstraZeneca, and Eli Lilly. In addition, he has received honoraria for consultant/advisory roles from Celgene, Moderna Therapeutics, Shattuck Labs, Pierre-Fabre, AstraZeneca, EMD Serono, Ono Pharmaceuticals, Clinica Alemana de Santiago, Dynamo Therapeutics, PeerView, Abbvie, Fluidigm, Takeda/Millenium Pharmaceuticals, Merck, Bristol-Myers Squibb, Agenus, and Torque Therapeutics. D.L.R. has served as an advisor for AstraZeneca, Agendia, Amgen, BMS, Cell Signaling Technology, Cepheid, Danaher, Daiichi Sankyo, Novartis, GSK, Konica Minolta, Merck, NanoString, PAIGE.AI, Perkin Elmer, Regeneron, Roche, Sanofi, Ventana and Ultivue. Amgen, Cepheid, Konica Minolta, NavigateBP, NextCure, and Lilly have funded research in his lab. V.B., D.B., and M.B. are currently employees of Bristol-Myers Squibb. S.B. received research funding from Roche and Basilea (to institution) and has served as a scientific advisory board member for Eli Lilly. The remaining authors declare no competing interests.
Figures


References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
