

Positive antiphospholipid antibodies: observation or treatment?
- PMID: 37264223
- PMCID: PMC10234248
- DOI: 10.1007/s11239-023-02834-6
Positive antiphospholipid antibodies: observation or treatment?
Abstract
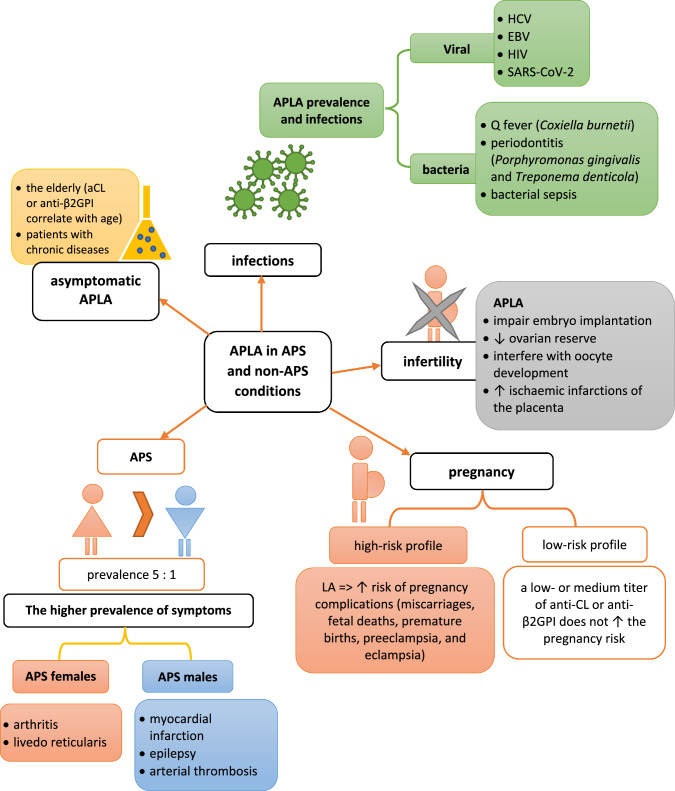
Antiphospholipid antibodies (APLAs) are primarily directed toward phospholipid-binding proteins and are responsible for thrombotic events. APLAs include anti-β2Glycoprotein I (anti-β2GPI), anticardiolipin (anti-CL) antibodies, and lupus anticoagulant. These antibodies are typical markers of antiphospholipid syndrome (APS) and are a part of its diagnostic criteria. Many data underline the presence of APLAs in other rheumatic diseases (e.g., systemic lupus erythematosus, systemic sclerosis, Sjögren's syndrome, rheumatoid arthritis and Behçet's disease). However, they are also detected in patients with cancer, infection, and neurological disorders. Furthermore, healthy individuals may be carriers of APLAs. Chronic asymptomatic APLAs presence is most common in the elderly and subjects with chronic diseases (including malignancies). Specific kinds of APLAs are considered markers of oncological progression. These antibodies occur in 6% of pregnant women (without diagnosed APS) and are related to many pregnancy complications. Of worth, various types of APLAs are reported to have different prothrombotic properties. The risk of thrombotic events in APLA-positive but clinically naïve patients raises many questions in clinical practice. This manuscript analyses various clinical situations and consequences of the APLAs' presence, particularly in patients without diagnosed APS. The prevalence, etiology, molecular background, and prothrombotic properties of numerous APLAs are broadly discussed. The new management approach in different clinical conditions and organ complications is present in the context of recent recommendations. Discussed data underlines that adequate and timely introduced thromboprophylaxis can decrease the risk of thrombus formation and prevent increased morbidity.
Keywords: APLAs in a healthy population; Antiphospholipid antibodies; Molecular mechanisms; Rheumatic and non-rheumatic diseases; Treatment.
© 2023. The Author(s).
Conflict of interest statement
None declared.
Figures

References
-
- Girón-González JA, García del Río E, Rodríguez C, et al. Antiphospholipid syndrome and asymptomatic carriers of antiphospholipid antibody: prospective analysis of 404 individuals. J Rheumatol. 2004;31:1560–1567. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
