

Management and Outcomes of Wilms Tumor With Suprarenal Intravascular Extension: A Pediatric Surgical Oncology Research Collaborative Study
- PMID: 37264925
- PMCID: PMC10829895
- DOI: 10.1097/SLA.0000000000005921
Management and Outcomes of Wilms Tumor With Suprarenal Intravascular Extension: A Pediatric Surgical Oncology Research Collaborative Study
Abstract
Objective: The purpose of this study was to describe management and outcomes from a contemporary cohort of children with Wilms tumor complicated by inferior vena caval thrombus.
Background: The largest series of these patients was published almost 2 decades ago. Since then, neoadjuvant chemotherapy has been commonly used to manage these patients, and outcomes have not been reported.
Methods: Retrospective review of 19 North American centers between 2009 and 2019. Patient and disease characteristics, management, and outcomes were investigated and analyzed.
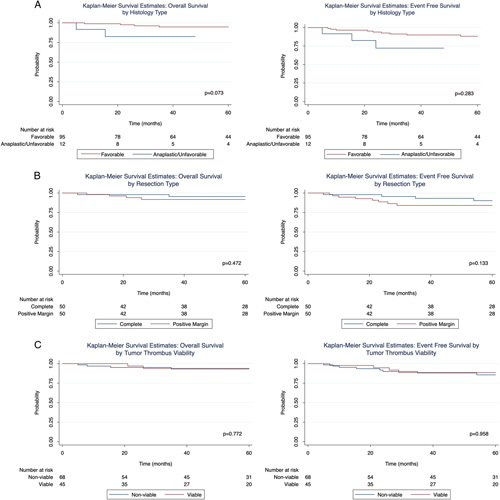
Results: Of 124 patients, 81% had favorable histology (FH), and 52% were stage IV. IVC thrombus level was infrahepatic in 53 (43%), intrahepatic in 32 (26%), suprahepatic in 14 (11%), and cardiac in 24 (19%). Neoadjuvant chemotherapy using a 3-drug regimen was administered in 82% and postresection radiation in 90%. Thrombus level regression was 45% overall, with suprahepatic level showing the best response (62%). Cardiopulmonary bypass (CPB) was potentially avoided in 67%. The perioperative complication rate was significantly lower after neoadjuvant chemotherapy [(25%) vs upfront surgery (55%); P =0.005]. CPB was not associated with higher complications [CPB (50%) vs no CPB (27%); P =0.08]. Two-year event-free survival was 93% and overall survival was 96%, higher in FH cases (FH 98% vs unfavorable histology/anaplastic 82%; P =0.73). Neither incomplete resection nor viable thrombus cells affected event-free survival or overall survival.
Conclusions: Multimodal therapy resulted in excellent outcomes, even with advanced-stage disease and cardiac extension. Neoadjuvant chemotherapy decreased the need for CPB to facilitate resection. Complete thrombectomy may not always be necessary.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures




References
-
- Pastore G, Znaor A, Spreafico F, et al. . Malignant renal tumours incidence and survival in European children (1978-1997): report from the Automated Childhood Cancer Information System project. Eur J Cancer. 2006;42:2103–2114. - PubMed
-
- Cunningham ME, Klug TD, Nuchtern JG, et al. . Global disparities in Wilms tumor. J Surg Res. 2020;247:34–51. - PubMed
-
- Dzhuma K, Powis M, Vujanic G, et al. . Surgical management, staging, and outcomes of Wilms tumours with intravascular extension: results of the IMPORT study. J Pediatr Surg. 2022;57:572–578. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
