

Total Synovectomy and Bone Grafting/Cementation after Curettage of the Bone Lesion in Diffuse Type of Tenosynovial Giant Cell Tumor: A Retrospective Cohort Study
- PMID: 37265527
- PMCID: PMC10231917
- DOI: 10.22038/ABJS.2023.67493.3203
Total Synovectomy and Bone Grafting/Cementation after Curettage of the Bone Lesion in Diffuse Type of Tenosynovial Giant Cell Tumor: A Retrospective Cohort Study
Abstract
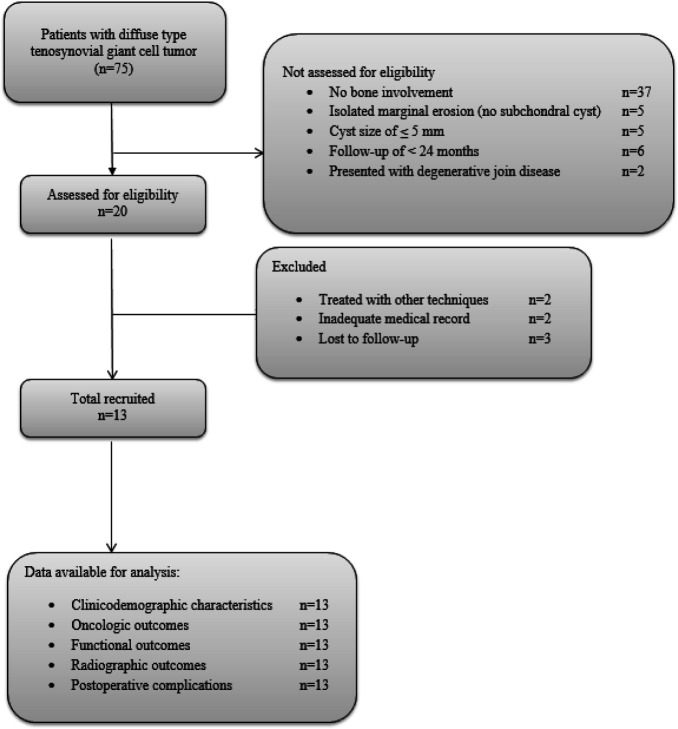
Objectives: Although the diffuse type of tenosynovial giant cell tumor (D-TGCT) is rare, bone involvement is common in such lesions. However, the optimal management of bone lesions in D-TGCT is not well-described. In this study, we reported the outcomes of total synovectomy, curettage, and bone grafting/cementation in the treatment of D-TGCT with subchondral bone involvement. We also described the prevalence, demographic, and characteristic features of the lesions.
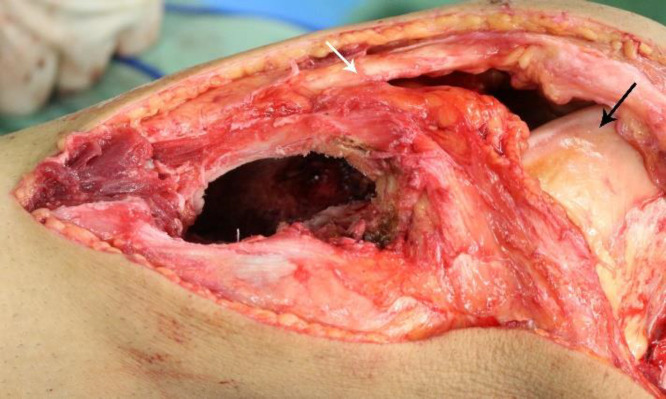
Methods: In a retrospective study, we included 13 patients with D-TGCT of large joints and associated subchondral cyst/cyst-like bone lesions of ≥ 5 mm that were managed with total synovectomy and curettage. Cavities with a bone defect of ≤ 30 mm (n=12) were filled with bone grafts. Cavities of > 30 mm (n=1) were augmented with bone cement. The limb function was evaluated by the Musculoskeletal Tumor Society (MSTS) score.
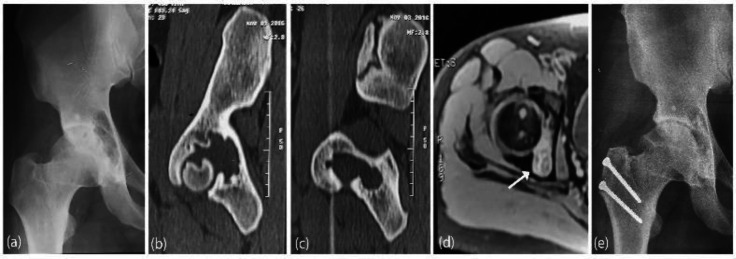
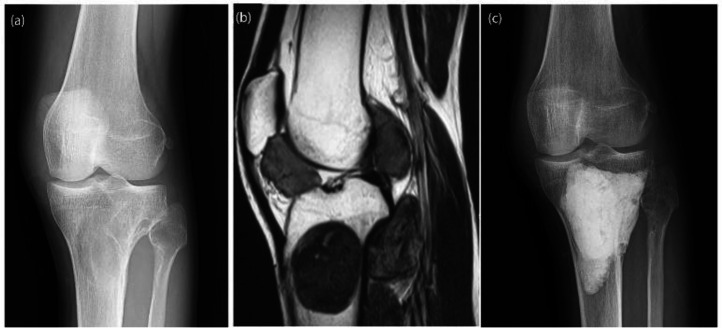
Results: The study population consisted of 6 (46.1%) males and 7 (53.9%) females with a mean age of 30 ± 7.9 years. The most frequent sites of involvement were the knees and ankle joints (n=5 each, 38.5%). The mean follow-up of the patients was 69.2 ± 32.9 months. The mean MSTS score of the patients was obtained at 98.2 ± 3.2 (range 90-100). The D-TGCT recurred in two patients, both of which were in the synovium. Postoperative complications were three cases of transient pain and one case of knee joint stiffness. While no patient had an osteoarthritic change in preoperative radiographs, two patients had osteoarthritic change (grade II) in the last follow-up, one in the knee and one in the hip.
Conclusion: Curettage and filling the defect with bone graft or cement are adequate treatments for managing bone lesions in D-TGCT.
Keywords: Bone lesion; Curettage; Diffuse tenosynovial giant cell tumor; Pigmented villonodular synovitis.
Conflict of interest statement
None
Figures
Similar articles
-
Extensile Anterior and Posterior Knee Exposure for Complete Synovectomy of Diffuse Tenosynovial Giant Cell Tumor (Pigmented Villonodular Synovitis).JBJS Essent Surg Tech. 2022 May 25;12(2):e21.00035. doi: 10.2106/JBJS.ST.21.00035. eCollection 2022 Apr-Jun. JBJS Essent Surg Tech. 2022. PMID: 36741035 Free PMC article.
-
Distinct extra-articular invasion patterns of diffuse pigmented villonodular synovitis/tenosynovial giant cell tumor in the knee joints.Knee Surg Sports Traumatol Arthrosc. 2018 Nov;26(11):3508-3514. doi: 10.1007/s00167-018-4942-2. Epub 2018 Apr 10. Knee Surg Sports Traumatol Arthrosc. 2018. PMID: 29637236
-
Midterm outcomes of 18 patients with primary intra-articular diffuse tenosynovial giant cell tumor (TGCT) of the knee treated with complete arthroscopic synovectomy and postoperative low-dose radiotherapy at a mean follow-up of 68 months.Arch Orthop Trauma Surg. 2023 Apr;143(4):2121-2127. doi: 10.1007/s00402-022-04465-7. Epub 2022 May 14. Arch Orthop Trauma Surg. 2023. PMID: 35562595
-
MRI of diffuse-type tenosynovial giant cell tumour in the knee: a guide for diagnosis and treatment response assessment.Insights Imaging. 2023 Feb 1;14(1):22. doi: 10.1186/s13244-023-01367-z. Insights Imaging. 2023. PMID: 36725759 Free PMC article. Review.
-
Current Systemic Treatment Options for Tenosynovial Giant Cell Tumor/Pigmented Villonodular Synovitis: Targeting the CSF1/CSF1R Axis.Curr Treat Options Oncol. 2016 Feb;17(2):10. doi: 10.1007/s11864-015-0385-x. Curr Treat Options Oncol. 2016. PMID: 26820289 Review.
Cited by
-
Invasion Patterns and Long-Term Clinical Outcomes of Diffuse Tenosynovial Giant Cell Tumor of the Ankle Joint.Cureus. 2024 Mar 14;16(3):e56148. doi: 10.7759/cureus.56148. eCollection 2024 Mar. Cureus. 2024. PMID: 38487651 Free PMC article.
References
-
- Myers BW, Masi AT, FEIGENBAUM SL. Pigmented villonodular synovitis and tenosynovitis: a clinical epidemiologic study of 166 cases and literature review. Medicine (Baltimore). 1980;59(3):223–238. - PubMed
-
- Ogilvie-Harris D, McLean J, Zarnett M. Pigmented villonodular synovitis of the knee The results of total arthroscopic synovectomy, partial, arthroscopic synovectomy, and arthroscopic local excision. J Bone Joint Surg Am. 1992;74(1):119–123. - PubMed
-
- Palmerini E, Staals EL, Maki RG, et al. Tenosynovial giant cell tumour/pigmented villonodular synovitis: outcome of 294 patients before the era of kinase inhibitors. Eur J Cancer. 2015;51(2):210–217. - PubMed
-
- Dorwart RH, Genant HK, Johnston WH, Morris JM. Pigmented villonodular synovitis of synovial joints: clinical, pathologic, and radiologic features. Am J Roentgenol. 1984;143(4):877–85. - PubMed
LinkOut - more resources
Full Text Sources