

A process mining approach for clinical guidelines compliance: real-world application in rectal cancer
- PMID: 37265796
- PMCID: PMC10231435
- DOI: 10.3389/fonc.2023.1090076
A process mining approach for clinical guidelines compliance: real-world application in rectal cancer
Abstract
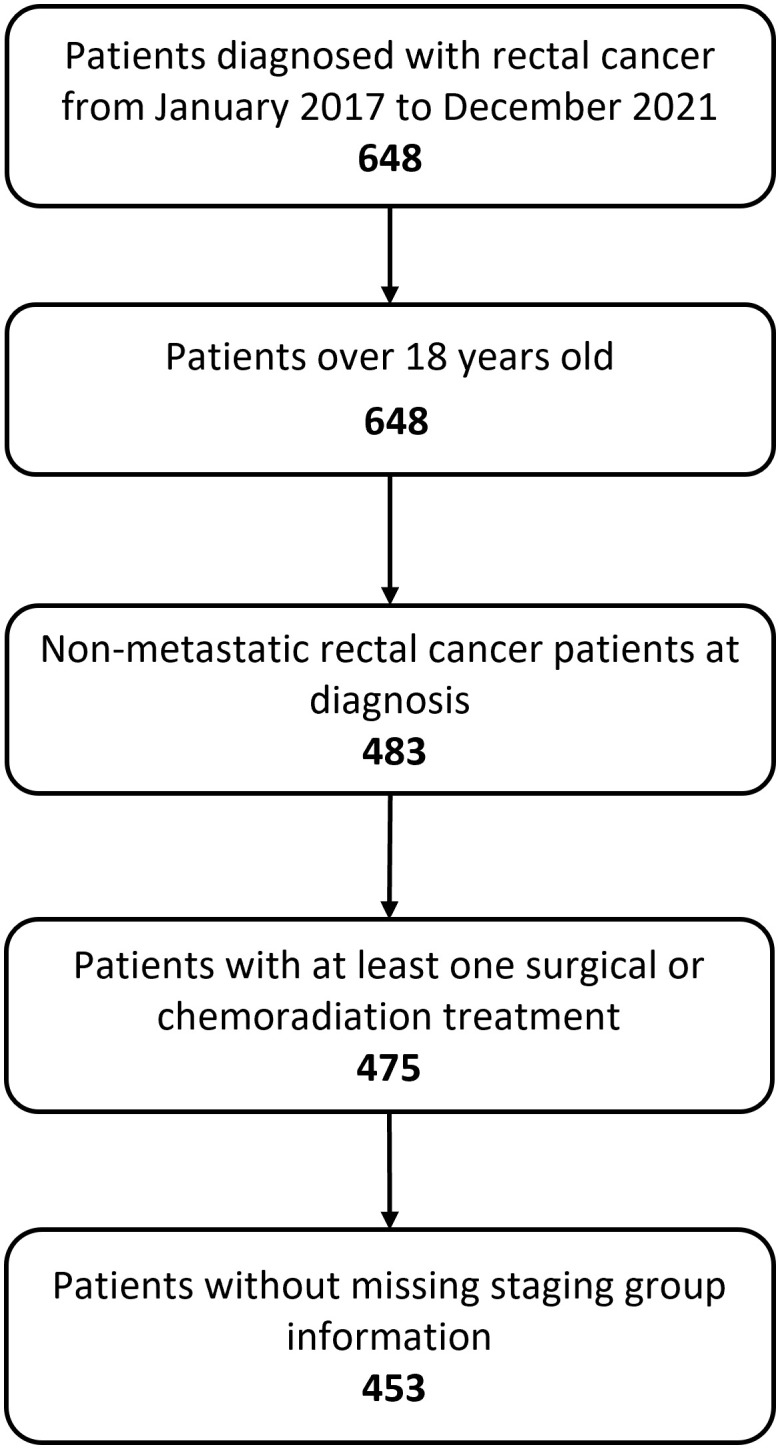
In the era of evidence-based medicine, several clinical guidelines were developed, supporting cancer management from diagnosis to treatment and aiming to optimize patient care and hospital resources. Nevertheless, individual patient characteristics and organizational factors may lead to deviations from these standard recommendations during clinical practice. In this context, process mining in healthcare constitutes a valid tool to evaluate conformance of real treatment pathways, extracted from hospital data warehouses as event log, to standard clinical guidelines, translated into computer-interpretable formats. In this study we translate the European Society of Medical Oncology guidelines for rectal cancer treatment into a computer-interpretable format using Pseudo-Workflow formalism (PWF), a language already employed in pMineR software library for Process Mining in Healthcare. We investigate the adherence of a real-world cohort of rectal cancer patients treated at Fondazione Policlinico Universitario A. Gemelli IRCCS, data associated with cancer diagnosis and treatment are extracted from hospital databases in 453 patients diagnosed with rectal cancer. PWF enables the easy implementation of guidelines in a computer-interpretable format and visualizations that can improve understandability and interpretability of physicians. Results of the conformance checking analysis on our cohort identify a subgroup of patients receiving a long course treatment that deviates from guidelines due to a moderate increase in radiotherapy dose and an addition of oxaliplatin during chemotherapy treatment. This study demonstrates the importance of PWF to evaluate clinical guidelines adherence and to identify reasons of deviations during a treatment process in a real-world and multidisciplinary setting.
Keywords: clinical guidelines; computer-interpretable clinical guidelines; conformance checking; evidence - based medicine; process discovery; process mining; rectal cancer; treatment pathways.
Copyright © 2023 Savino, Chiloiro, Masciocchi, Capocchiano, Lenkowicz, Gottardelli, Gambacorta, Valentini and Damiani.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures






References
-
- Chiloiro G, Cusumano D, de Franco P, Lenkowicz J, Boldrini L, Carano D, et al. . Does restaging MRI radiomics analysis improve pathological complete response prediction in rectal cancer patients? a prognostic model development. Radiol Med (2022) 127(1):11–20. doi: 10.1007/s11547-021-01421-0 - DOI - PubMed
LinkOut - more resources
Full Text Sources