

Autoimmune Polyendocrinopathy in a Pediatric Patient Presenting With Multisystem Inflammatory Syndrome in Children (MIS-C)
- PMID: 37265890
- PMCID: PMC10232015
- DOI: 10.7759/cureus.38407
Autoimmune Polyendocrinopathy in a Pediatric Patient Presenting With Multisystem Inflammatory Syndrome in Children (MIS-C)
Abstract
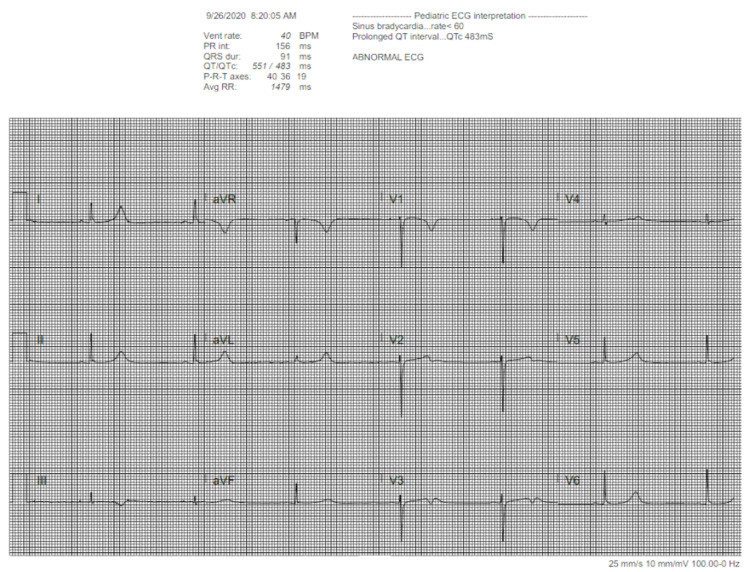
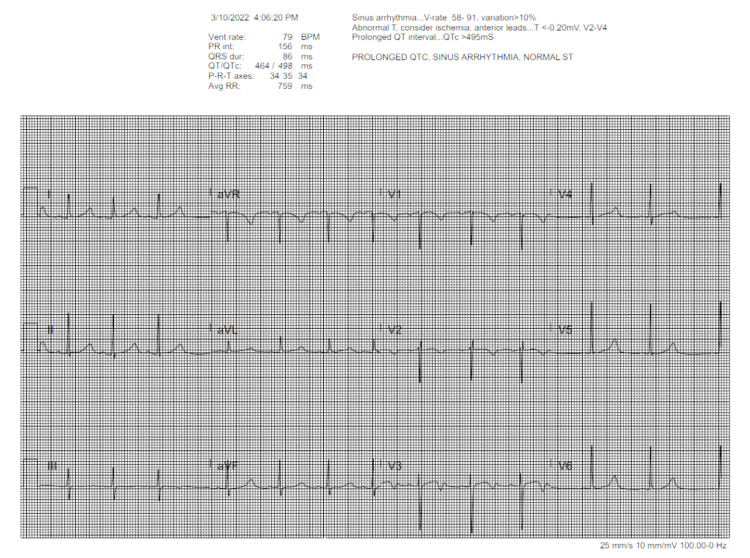
Multisystem inflammatory syndrome (MIS) is a well-known potential sequela of COVID-19 infection. Though prevalence is higher in certain populations, this syndrome is a rare occurrence in children. Beyond MIS, there has been increasing research into COVID infection and the subsequent onset of autoimmune conditions, such as diabetes. However, evidence of a poly-endocrinopathy developing after COVID infection is lacking, and evidence within the pediatric population is virtually nonexistent. In this case, we present the evolution of an autoimmune polyglandular syndrome (APS) type 2 phenotype, consisting of type 1 diabetes, Graves' disease, and adrenal insufficiency, after diagnosis of multisystem inflammatory syndrome of children (MIS-C) in a pediatric patient. A 15-year-old biracial female without significant past medical history tested positive for COVID-19 and two weeks later presented with respiratory symptoms and other systemic signs. She was admitted for further evaluation and was found to have elevated inflammatory markers, EKG (electrocardiogram) abnormalities, and lab evidence of organ damage. The patient was diagnosed with MIS-C, and treatment was initiated with eventual discharge. One year after this initial visit, the patient returned to the hospital due to weight loss, difficulty breathing, polyuria, polydipsia, nausea, vomiting, and fatigue. A steroid course for MIS-C treatment had been completed three months prior. Exam and lab results confirmed diabetic ketoacidosis (DKA), and the patient was diagnosed with new-onset type 1 diabetes. Further testing determined that she was glutamic acid decarboxylase 65 (GAD-65) positive. DKA was managed in the hospital, and the patient was subsequently discharged with an insulin regimen and endocrine follow-up. A couple of months later, the patient returned to the emergency department (ED) due to two weeks of dyspnea on exertion and dizziness. Since her previous admission for DKA, the patient had contracted COVID-19 again and recovered from her respiratory symptoms. Physical exam and labs were grossly unremarkable; however, the patient had EKG abnormalities and an episode of severe bradycardia, prompting hospitalization. Thyroid workup revealed thyrotoxicosis due to Graves' disease. Due to intermittent hypotension, adrenal labs were obtained. She was found to have adrenal insufficiency as well, with a positive 21-hydroxylase antibody. Throughout these hospitalizations, the patient suffered from skin and hair changes as well, ultimately requiring dermatological intervention.
Keywords: addison's disease; aps type ii; autoimmune polyendocrine syndrome ii; covid-19; endocrine disorders; graves' disease; multi-system inflammatory syndrome in children (mis-c); pediatric case; type i diabetes mellitus.
Copyright © 2023, Sambangi et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
New-Onset Primary Adrenal Insufficiency and Autoimmune Hypothyroidism in a Pediatric Patient Presenting with MIS-C.Horm Res Paediatr. 2022;95(4):397-401. doi: 10.1159/000525227. Epub 2022 May 24. Horm Res Paediatr. 2022. PMID: 35609533 Free PMC article.
-
Management of Adrenal Deficiency and Shock in a Patient With Polyglandular Autoimmune Syndrome Type II.Cureus. 2023 Jul 6;15(7):e41440. doi: 10.7759/cureus.41440. eCollection 2023 Jul. Cureus. 2023. PMID: 37546049 Free PMC article.
-
Multisystem Inflammatory Syndrome in Children (MIS-C) in an Adolescent that Developed Coronary Aneurysms: A Case Report and Review of the Literature.J Emerg Med. 2020 Nov;59(5):699-704. doi: 10.1016/j.jemermed.2020.09.008. Epub 2020 Oct 1. J Emerg Med. 2020. PMID: 33011038 Free PMC article. Review.
-
New-onset diabetic ketoacidosis with purpura fulminans in a child with COVID-19-related multisystem inflammatory syndrome.Infect Dis (Lond). 2022 Jul;54(7):522-528. doi: 10.1080/23744235.2022.2050423. Epub 2022 Mar 17. Infect Dis (Lond). 2022. PMID: 35300573
-
Autoimmune polyglandular syndrome type II with co-manifestation of Addison's and Graves' disease in a 15-year-old boy: case report and literature review.J Pediatr Endocrinol Metab. 2020 Apr 28;33(4):575-578. doi: 10.1515/jpem-2019-0506. J Pediatr Endocrinol Metab. 2020. PMID: 32112702 Review.
Cited by
-
The multiple faces of autoimmune Addison's disease in children.Front Endocrinol (Lausanne). 2024 Sep 16;15:1411774. doi: 10.3389/fendo.2024.1411774. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39351530 Free PMC article. Review.
References
-
- Son MBF, Friedman K. UpToDate. Waltham, MA: UpToDate; 2023. COVID-19: Multisystem inflammatory syndrome in children (MIS-C) clinical features, evaluation, and diagnosis.
-
- COVID-19 trends among persons aged 0-24 years - United States, March 1-December 12, 2020. Leidman E, Duca LM, Omura JD, Proia K, Stephens JW, Sauber-Schatz EK. http://dx.doi.org/10.15585/mmwr.mm7003e1external. MMWR Morb Mortal Wkly Rep. 2021;70:88–94. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous