

Case Reports
doi: 10.1016/j.radcr.2023.05.015.
eCollection 2023 Aug.
An Atypical presentation of pulmonary embolism in a critically ill patient
Affiliations
- PMID: 37266377
- PMCID: PMC10230824
- DOI: 10.1016/j.radcr.2023.05.015
Item in Clipboard
Case Reports
An Atypical presentation of pulmonary embolism in a critically ill patient
Radiol Case Rep.
.
Abstract
A pulmonary embolism (PE) occurs when a venous thrombotic material from the lower extremities embolizes to the pulmonary vasculature. Common presenting symptoms include shortness of breath and pleuritic chest pain with vital signs demonstrating hypoxia, tachycardia, and tachypnea. In this paper, we describe a unique presentation of a critically ill patient who developed a saddle pulmonary embolism despite being on prophylactic anticoagulation.
Keywords: Anticoagulation; Computer tomographic pulmonary angiography; Hypoxia; Pulmonary embolism.
© 2023 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures
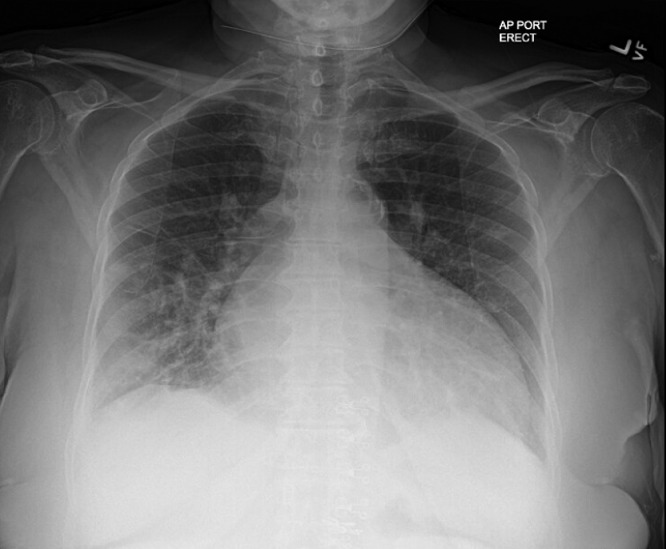
Chest radiograph (day 1 on admission) with ground glass air opacities in the right lung base.

Repeat chest radiograph (day 4 of admission) demonstrating increased density of air opacities in the right lung base.
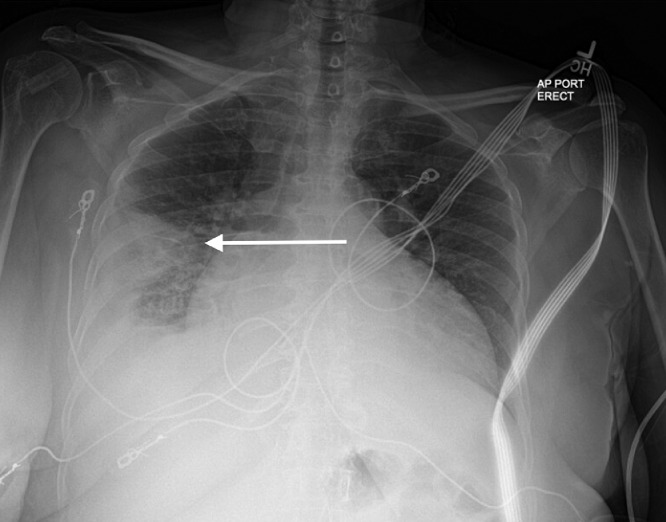
Follow up chest radiograph (day 5 of admission) showing wedge shaped peripheral opacity in the right middle lung (white arrow) with associated effusion and atelectasis, concerning for pneumonia or pulmonary embolism.
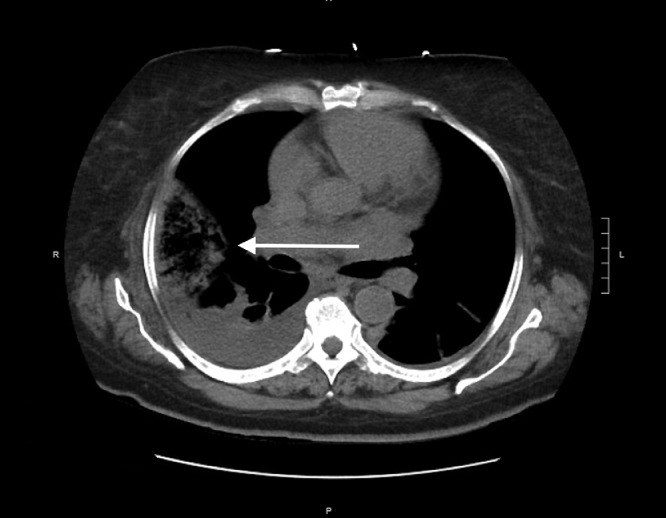
Computer tomography of the chest (day 5 of admission) revealing dome shaped opacities in the right middle and right lower lobes (white arrow), which could represent pneumonia or pulmonary infarction. Bilateral, right worse than left, pleural effusions are also noted.

(A–C) Computer tomographic pulmonary angiography (day 5 of admission) revealing massive saddle pulmonary embolus (white arrow). Bilateral, right worse than left, pleural effusions are also noted.
References
Publication types
LinkOut - more resources
Full Text Sources
