

Stenting or angioplasty for the treatment of deep vein thrombosis: Systematic review and meta-analysis of randomized controlled trials
- PMID: 37266612
- PMCID: PMC10237682
- DOI: 10.1097/MD.0000000000033924
Stenting or angioplasty for the treatment of deep vein thrombosis: Systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Although the cornerstone treatment for deep vein thrombosis (DVT) remains anticoagulation, clinicians perform stenting or angioplasty (SA) in particular patients. To assess the effects of SA in this setting, we performed a systematic review of randomized controlled trials.
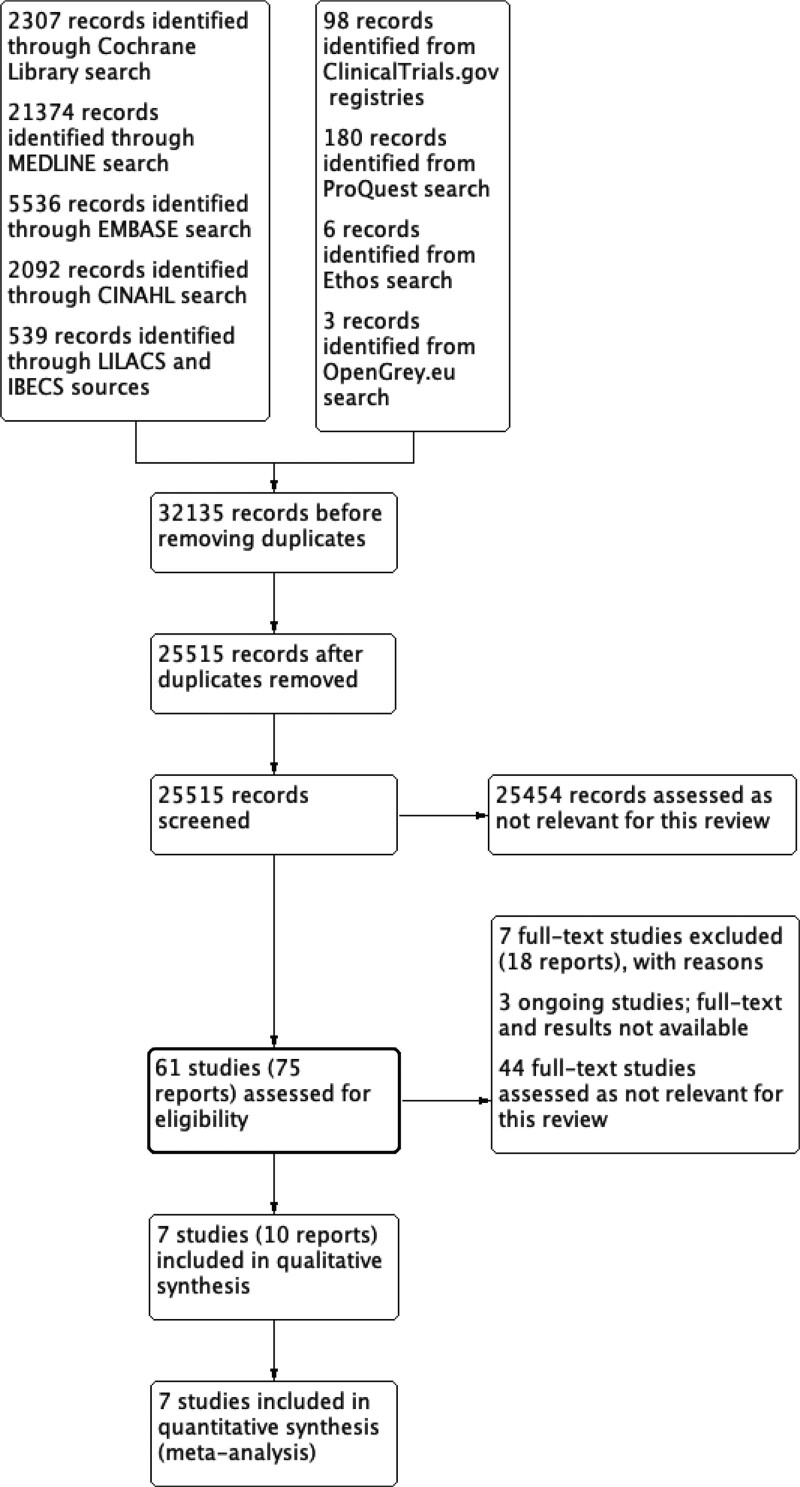
Methods: Based on the Cochrane standards, we searched the Cochrane CENTRAL, MEDLINE, Embase, CINAHL, LILACS and IBECS databases, and trial registries. Our primary outcomes were post-thrombotic syndrome (PTS), venous thromboembolism (VTE) and all-cause mortality.
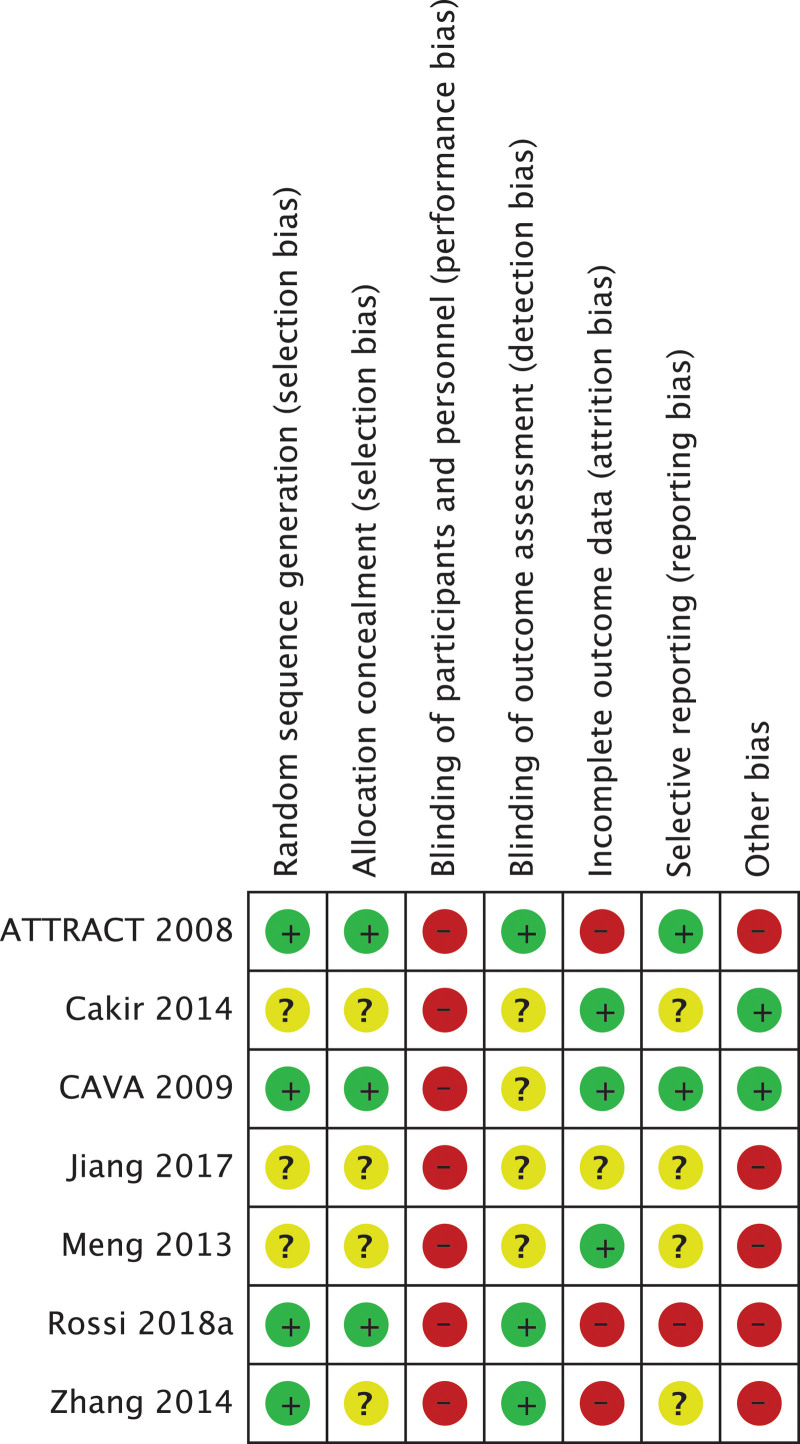
Results: We included 7 randomized controlled trial (1485 participants). There was no clinically significant difference between SA and best medical practice (BMP) for the additional treatment of acute DVT regarding PTS (standardized mean difference -7.87, 95% confidence interval [CI] -12.13 to -3.61; very low-certainty) and VTE (risk ratio [RR] 1.19, 95% CI 0.28-5.07, very low-certainty), and no deaths. Compared to BMP, the SA plus BMP and thrombolysis results in little to no difference in PTS (mean difference [MD] -1.07, 95% CI -1.12 to -1.02, moderate-certainty), VTE (RR 1.48, 95% CI 0.95-2.31, low-certainty), and mortality (RR 0.92, 95% CI 0.34-2.52, low-certainty). There was no clinical difference between stenting and BMP for chronic DVT regarding PTS (MD 2.73, 95% CI -2.10 to 7.56, very low certainty) and no VTE and death events.
Conclusions: SA results in little to no difference in PTS, VTE and mortality in acute DVT compared to BMP. The evidence regarding SA in chronic DVT and whether SA, compared to BMP and thrombolysis, decreases PTS and VTE in acute DVT is uncertain. Open Science Framework (osf.io/f2dm6).
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc.
Figures
References
-
- Kakkos SK, Gohel M, Baekgaard N, et al. . Clinical practice guidelines on the management of venous thrombosis. Eur J Vasc Endovasc Surg. 2021;61:9–82. - PubMed
-
- Di Nisio M, van Es N, Büller HR. Deep vein thrombosis and pulmonary embolism. Lancet. 2016;388:3060–73. - PubMed
-
- Stevens SM, Woller SC, Kreuziger LB, et al. . Antithrombotic therapy for VTE disease: second update of the CHEST guideline and expert panel report. Chest. 2021;160:e545–608. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
