

Gestational trophoblastic neoplasia mimicking ruptured ectopic pregnancy: A case report
- PMID: 37266616
- PMCID: PMC10238010
- DOI: 10.1097/MD.0000000000033947
Gestational trophoblastic neoplasia mimicking ruptured ectopic pregnancy: A case report
Abstract
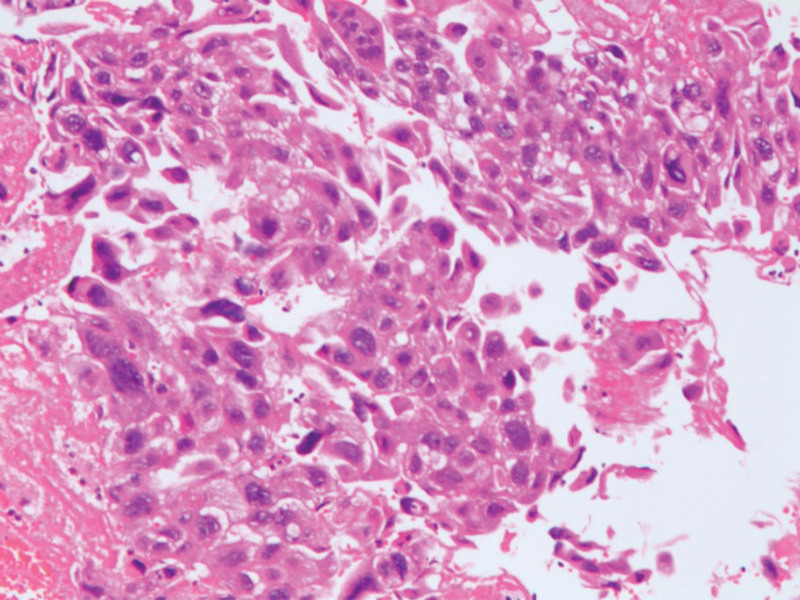
Rationale: Gestational trophoblastic neoplasia (GTN) refers to the hydatidiform mole tissue that invades the myometrium or even penetrates the uterine wall to the broad ligament or abdominal cavity, and a few have distant metastases through blood transport. According to the World Health Organization[1] 2020 (5th edition) classification lists an erosive hydatidiform mole as a borderline or biologically behavioral uncertain tumor, it continues to be clinically classified as a malignancy and combined with choriocarcinoma as a GTN. The clinical manifestations of GTN include amenorrhea, abnormal vaginal bleeding, and increased serum human chorionic gonadotropin level, which are also common clinical features of ectopic pregnancy. The diagnosis of typical GTN is not difficult. However, some patients with atypical clinical manifestations and a lack of specificity in their B-ultrasound images are easy to misdiagnose, especially when the lesions are located in special parts outside the uterus and lack specific imaging features.
Patient concerns: A 41-year-old woman who presented 3 months after having an abortion with severe abdominal pain that lasted 15 hours.
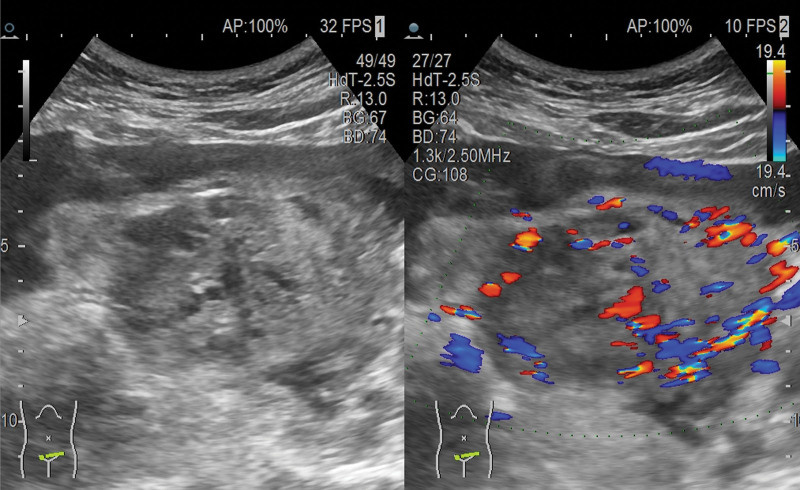
Diagnoses: CT showed massive blood accumulation in the abdominal cavity and the pelvic cavity. Uterine lesions? Transvaginal uterine ultrasound reveals: a right intrauterine mixed mass (approximately 83 * 66 mm mixed echo mass), a possible pregnancy, and a rupture pregnancy (right pregnancy). abdominal effusion (large) and clots, maximum front and rear diameters of 95 mm, pelvic effusion, and about 20 mm deep. HCG levels in the blood were 17,452 IU/L and hemoglobin levels were 81 g/L. Admission diagnosis: Abdominal pain investigation: ectopic pregnancy? Bleeding shock.
Interventions: Laparoscopy and laparotomy followed by hysterectomy, treated by chemotherapy.
Outcomes: Hysterectomy was required due to intraoperative hemostasis difficulties, and the patient lost her uterus forever.
Lessons: Continued reporting of these cases are important so that the gynecologists are aware about the possibility of ruptured invasive mole and it should be kept as a differential diagnosis in all the pregnant women presents with acute onset lower abdominal pain.
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures


Similar articles
-
Invasive mole with lung metastasis after an abdominal complete hydatidiform mole treatment.J Obstet Gynaecol Res. 2021 Jan;47(1):420-424. doi: 10.1111/jog.14537. Epub 2020 Oct 20. J Obstet Gynaecol Res. 2021. PMID: 33078868
-
Ruptured large ectopic hydatidiform mole: an infrequent presentation of gestational trophoblastic disease.J Ultrasound. 2024 Dec;27(4):941-945. doi: 10.1007/s40477-024-00946-0. Epub 2024 Aug 5. J Ultrasound. 2024. PMID: 39102103
-
Gestational trophoblastic neoplasia after spontaneous human chorionic gonadotropin normalization following molar pregnancy evacuation.Gynecol Oncol. 2015 Nov;139(2):283-7. doi: 10.1016/j.ygyno.2015.09.012. Epub 2015 Sep 14. Gynecol Oncol. 2015. PMID: 26383828
-
Does a human chorionic gonadotropin level of over 20,000 IU/L four weeks after uterine evacuation for complete hydatidiform mole constitute an indication for chemotherapy for gestational trophoblastic neoplasia?Eur J Obstet Gynecol Reprod Biol. 2018 Apr;223:50-55. doi: 10.1016/j.ejogrb.2018.02.001. Epub 2018 Feb 15. Eur J Obstet Gynecol Reprod Biol. 2018. PMID: 29477553 Review.
-
Multiple metastatic gestational trophoblastic disease after a twin pregnancy with complete hydatidiform mole and coexisting fetus, following assisted reproductive technology: Case report and literature review.Taiwan J Obstet Gynecol. 2018 Aug;57(4):588-593. doi: 10.1016/j.tjog.2018.06.020. Taiwan J Obstet Gynecol. 2018. PMID: 30122584 Review.
Cited by
-
Gestational trophoblastic neoplasia with pulmonary embolism mimicking tuberculosis.J Family Med Prim Care. 2024 Mar;13(3):1115-1118. doi: 10.4103/jfmpc.jfmpc_1278_23. Epub 2024 Apr 4. J Family Med Prim Care. 2024. PMID: 38736792 Free PMC article.
References
-
- McCluggage WG, Singh N, Gilks CB. Key changes to the World Health Organization (WHO) classification of female genital tumours introduced in the 5th edition (2020). Histopathology. 2022;80:762–78. - PubMed
-
- Ngan HYS, Seckl MJ, Berkowitz RS, et al. . Update on the diagnosis and management of gestational trophoblastic disease. Int J Gynaecol Obstet. 2018;143(Suppl 2):79–85. - PubMed
-
- Hendriks E, Rosenberg R, Prine L. Ectopic pregnancy: diagnosis and management. Am Fam Physician. 2020;101:599–606. - PubMed
