

Primary biliary cholangitis: Epidemiology, prognosis, and treatment
- PMID: 37267215
- PMCID: PMC10241503
- DOI: 10.1097/HC9.0000000000000179
Primary biliary cholangitis: Epidemiology, prognosis, and treatment
Abstract
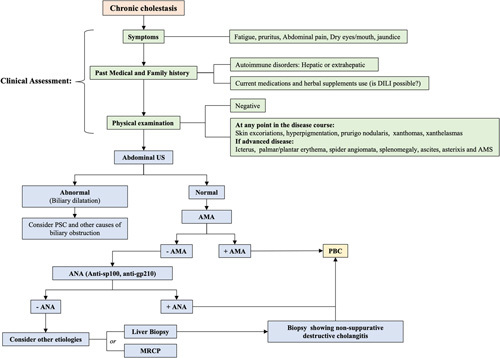
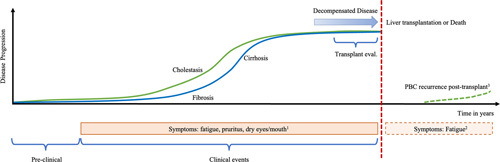
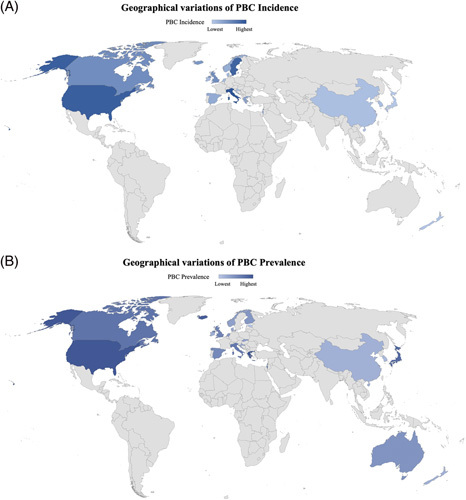
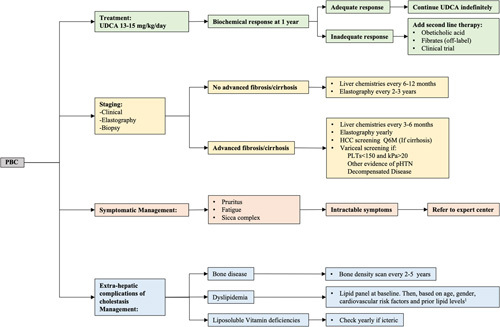
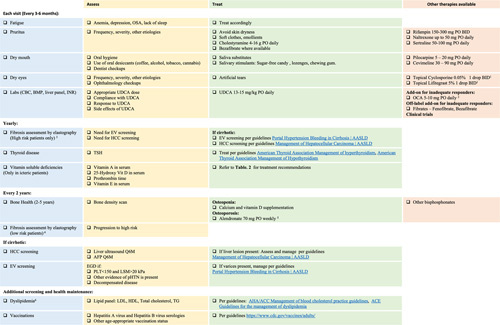
Primary biliary cholangitis (PBC) is a chronic cholestatic autoimmune liver disease characterized by a destructive, small duct, and lymphocytic cholangitis, and marked by the presence of antimitochondrial antibodies. The incidence and prevalence of PBC vary widely in different regions and time periods, and although disproportionally more common among White non-Hispanic females, contemporary data show a higher prevalence in males and racial minorities than previously described. Outcomes largely depend on early recognition of the disease and prompt institution of treatment, which, in turn, are directly influenced by provider bias and socioeconomic factors. Ursodeoxycholic acid remains the initial treatment of choice for PBC, with obeticholic acid and fibrates (off-label therapy) reserved as add-on therapy for the management of inadequate responders or those with ursodeoxycholic acid intolerance. Novel and repurposed drugs are currently at different stages of clinical development not only for the treatment of PBC but also for its symptomatic management. Here, we summarize the most up-to-date data regarding the epidemiology, prognosis, and treatment of PBC, providing clinically useful information for its holistic management.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Association for the Study of Liver Diseases.
Conflict of interest statement
Cynthia Levy consults and received grants from Calliditas, Cymabay, Genfit, Gilead, GlaxoSmithKline, Intercept, Mirum, and Target RWE. She consults for Ipsen and received grants from Cara, Escient, and Zydus. Binu John advises and is on the speakers’ bureau for GlaxoSmithKline. He advises AstraZeneca and received grants from Gilead, Exact Sciences, and Glycotest. The remaining author has no conflicts to report.
Figures
References
-
- Gulamhusein AF, Hirschfield GM. Primary biliary cholangitis: pathogenesis and therapeutic opportunities. Nat Rev Gastroenterol Hepatol. 2020;17:93–110. - PubMed
-
- Selmi C, Mayo MJ, Bach N, Ishibashi H, Invernizzi P, Gish RG, et al. Primary biliary cirrhosis in monozygotic and dizygotic twins: genetics, epigenetics, and environment. Gastroenterology. 2004;127:485–92. - PubMed
-
- Lazaridis KN, Juran BD, Boe GM, Slusser JP, de Andrade M, Homburger HA, et al. Increased prevalence of antimitochondrial antibodies in first-degree relatives of patients with primary biliary cirrhosis. Hepatology. 2007;46:785–92. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
