

Clinicoradiologic and Neuropathologic Evaluation of Corticobasal Syndrome
- PMID: 37268436
- PMCID: PMC10382268
- DOI: 10.1212/WNL.0000000000207397
Clinicoradiologic and Neuropathologic Evaluation of Corticobasal Syndrome
Abstract
Background and objectives: Corticobasal syndrome (CBS) is a clinical phenotype characterized by asymmetric parkinsonism, rigidity, myoclonus, and apraxia. Originally believed secondary to corticobasal degeneration (CBD), mounting clinicopathologic studies have revealed heterogenous neuropathologies. The objectives of this study were to determine the pathologic heterogeneity of CBS, the clinicoradiologic findings associated with different underlying pathologies causing CBS, and the positive predictive value (PPV) of current diagnostic criteria for CBD among patients with a CBS.
Methods: Clinical data, brain MRI, and neuropathologic data of patients followed at Mayo Clinic and diagnosed with CBS antemortem were reviewed according to neuropathology category at autopsy.
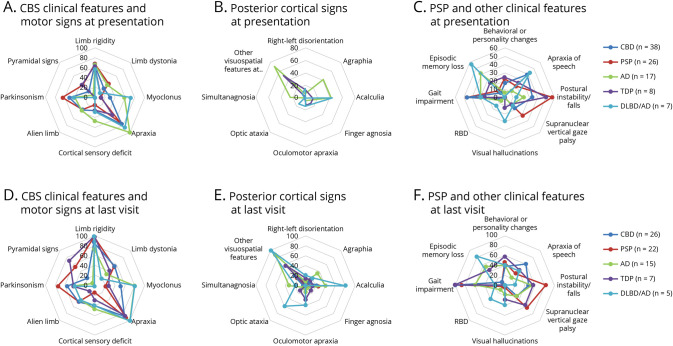
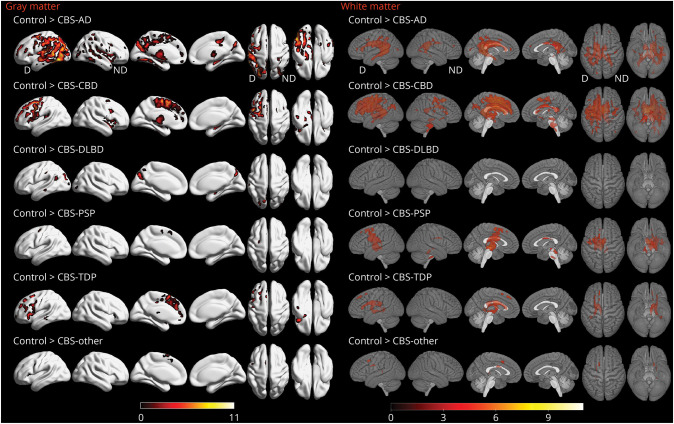
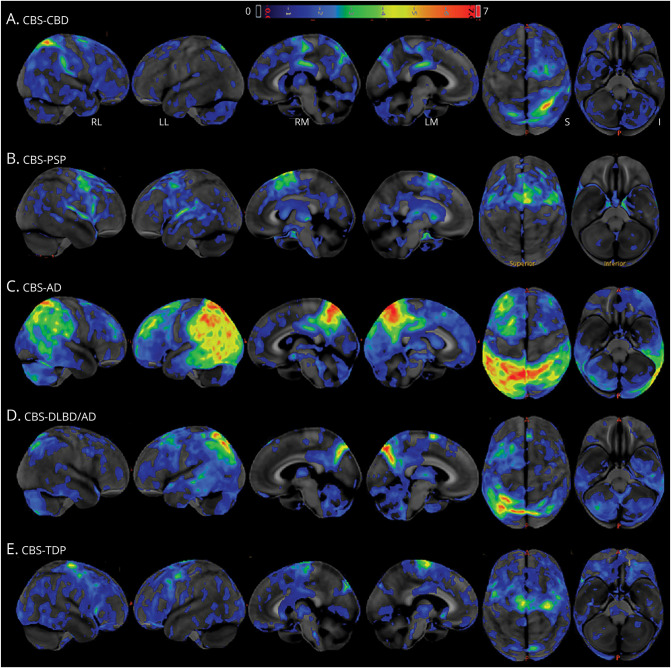
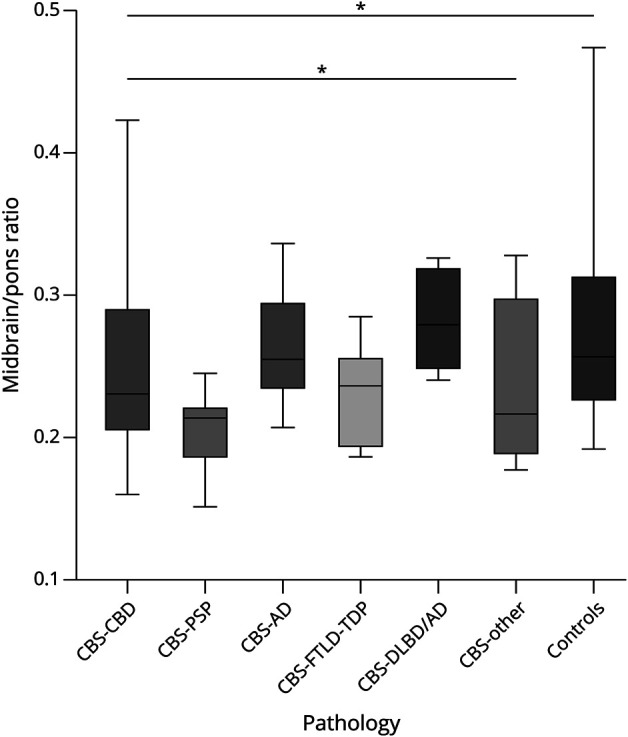
Results: The cohort consisted of 113 patients with CBS, 61 (54%) female patients. Mean ± SD disease duration was 7 ± 3.7 years; mean ± SD age at death was 70.5 ± 9.1 years. The primary neuropathologic diagnoses were 43 (38%) CBD, 27 (24%) progressive supranuclear palsy (PSP), 17 (15%) Alzheimer disease (AD), 10 (9%) frontotemporal lobar degeneration (FTLD) with TAR DNA-binding protein 43 (TDP) inclusions, 7 (6%) diffuse Lewy body disease (DLBD)/AD, and 9 (8%) with other diagnoses. Patients with CBS-AD or CBS-DLBD/AD were youngest at death (median [interquartile range]: 64 [13], 64 [11] years) while CBS-PSP were oldest (77 [12.5] years, p = 0.024). Patients with CBS-DLBD/AD had the longest disease duration (9 [6] years), while CBS-other had the shortest (3 [4.25] years, p = 0.04). Posterior cortical signs and myoclonus were more characteristic of patients with CBS-AD and patients with CBS-DLBD/AD. Patients with CBS-DLBD/AD displayed more features of Lewy body dementia. Voxel-based morphometry revealed widespread cortical gray matter loss characteristic of CBS-AD, while CBS-CBD and CBS-PSP predominantly involved premotor regions with greater amount of white matter loss. Patients with CBS-DLBD/AD showed atrophy in a focal parieto-occipital region, and patients with CBS-FTLD-TDP had predominant prefrontal cortical loss. Patients with CBS-PSP had the lowest midbrain/pons ratio (p = 0.012). Of 67 cases meeting clinical criteria for possible CBD at presentation, 27 were pathology-proven CBD, yielding a PPV of 40%.
Discussion: A variety of neurodegenerative disorders can be identified in patients with CBS, but clinical and regional imaging differences aid in predicting underlying neuropathology. PPV analysis of the current CBD diagnostic criteria revealed suboptimal performance. Biomarkers adequately sensitive and specific for CBD are needed.
© 2023 American Academy of Neurology.
Conflict of interest statement
D.S. Knopman serves on a Data Safety Monitoring Board for the DIAN study. He served on a Data Safety monitoring Board for a tau therapeutic for Biogen but receives no personal compensation. He is a site investigator in the Biogen aducanumab trials. He is an investigator in a clinical trial sponsored by Lilly Pharmaceuticals and the University of Southern California. He serves as a consultant for Samus Therapeutics, Roche, and Alzeca Biosciences but receives no personal compensation. R.C. Petersen serves as a consultant for Biogen, Inc., Roche, Inc., Merck, Inc., Genentech Inc. (DSMB), Nestle, Inc., and Eisai, Inc.; receives publishing royalties from Mild Cognitive Impairment (Oxford University Press, 2003) and UpToDate. B.F. Boeve, D.W. Dickson, K.A. Josephs, and J.L. Whitwell received research funding from the NIH and declare no competing financial interests. M.E. Murray is a consultant for AVID Radiopharmaceuticals. She receives support from the NIH/NIA and State of Florida. N.R. Graff-Radford receives royalties from UpToDate; has participated in multicenter therapy studies sponsored by Biogen, TauRx, AbbVie, Novartis, and Lilly; and he receives research support from NIH. J. Graff-Radford serves on the editorial board for
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous