

Distinguishing Distinct Neural Systems for Proximal vs Distal Upper Extremity Motor Control After Acute Stroke
- PMID: 37268437
- PMCID: PMC10435065
- DOI: 10.1212/WNL.0000000000207417
Distinguishing Distinct Neural Systems for Proximal vs Distal Upper Extremity Motor Control After Acute Stroke
Abstract
Background and objectives: The classic and singular pattern of distal greater than proximal upper extremity motor deficits after acute stroke does not account for the distinct structural and functional organization of circuits for proximal and distal motor control in the healthy CNS. We hypothesized that separate proximal and distal upper extremity clinical syndromes after acute stroke could be distinguished and that patterns of neuroanatomical injury leading to these 2 syndromes would reflect their distinct organization in the intact CNS.
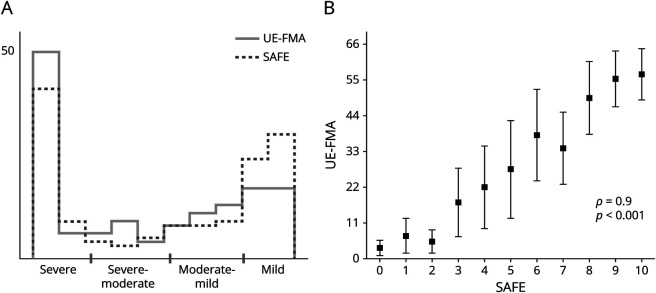
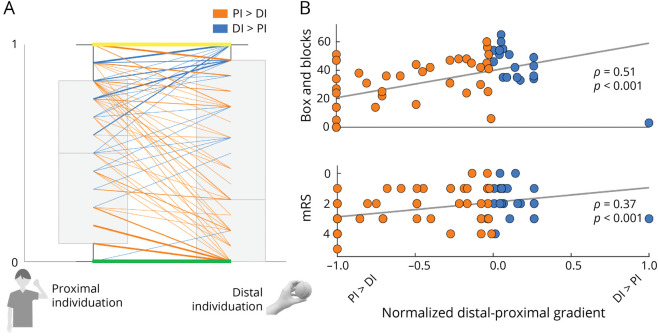
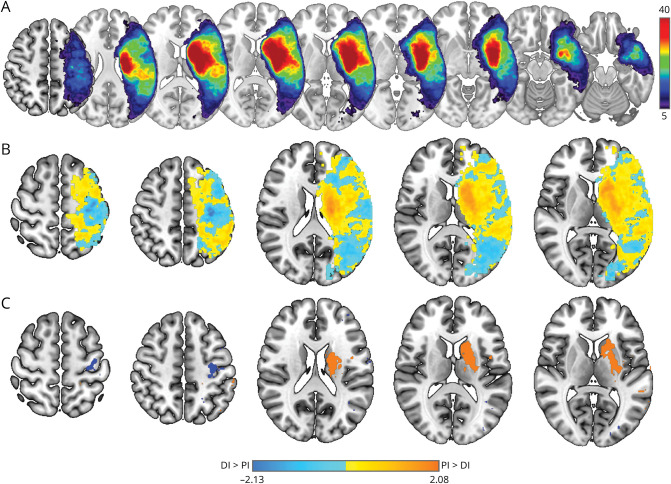
Methods: Proximal and distal components of motor impairment (upper extremity Fugl-Meyer score) and strength (Shoulder Abduction Finger Extension score) were assessed in consecutively recruited patients within 7 days of acute stroke. Partial correlation analysis was used to assess the relationship between proximal and distal motor scores. Functional outcomes including the Box and Blocks Test (BBT), Barthel Index (BI), and modified Rankin scale (mRS) were examined in relation to proximal vs distal motor patterns of deficit. Voxel-based lesion-symptom mapping was used to identify regions of injury associated with proximal vs distal upper extremity motor deficits.
Results: A total of 141 consecutive patients (49% female) were assessed 4.0 ± 1.6 (mean ± SD) days after stroke onset. Separate proximal and distal upper extremity motor components were distinguishable after acute stroke (p = 0.002). A pattern of proximal more than distal injury (i.e., relatively preserved distal motor control) was not rare, observed in 23% of acute stroke patients. Patients with relatively preserved distal motor control, even after controlling for total extent of deficit, had better outcomes in the first week and at 90 days poststroke (BBT, ρ = 0.51, p < 0.001; BI, ρ = 0.41, p < 0.001; mRS, ρ = 0.38, p < 0.001). Deficits in proximal motor control were associated with widespread injury to subcortical white and gray matter, while deficits in distal motor control were associated with injury restricted to the posterior aspect of the precentral gyrus, consistent with the organization of proximal vs distal neural circuits in the healthy CNS.
Discussion: These results highlight that proximal and distal upper extremity motor systems can be selectively injured by acute stroke, with dissociable deficits and functional consequences. Our findings emphasize how disruption of distinct motor systems can contribute to separable components of poststroke upper extremity hemiparesis.
Written work prepared by employees of the Federal Government as part of their official duties is, under the U.S. Copyright Act, a “work of the United States Government” for which copyright protection under Title 17 of the United States Code is not available. As such, copyright does not extend to the contributions of employees of the Federal Government.
Conflict of interest statement
D.J. Lin has served as a consultant for Boehringer Ingelheim and Neurotrauma Sciences and provides consultative input for The MGH Translational Research Center (on clinical research support agreements with BrainQ, Constant Therapy, Constant Therapeutics, Imago Rehab, and Reach Neuro). S.B. Snider is a site investigator on a Biogen-funded clinical trial that is unrelated to this work. K. Rishe provides consultative input for the MGH Translational Research Center (on a clinical research support agreement with Constant Therapeutics). L.R. Hochberg provides consultative input for the MGH Translational Research Center (on clinical research support agreements with Neuralink, Synchron, Reach Neuro, Axoft, and Precision Neuro). S.C. Cramer serves as a consultant for Abbvie, Constant Therapeutics, MicroTransponder, Neurolutions, SanBio, Panaxium, NeuExcell, Elevian, Medtronic, Helius, Omniscient, and TRCare. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Department of Veterans Affairs or the United States Government. Go to
Figures
Comment in
-
Challenging Historical Views in Stroke Recovery of the Upper Extremity: Out on a Limb.Neurology. 2023 Jul 25;101(4):149-150. doi: 10.1212/WNL.0000000000207499. Epub 2023 Jun 2. Neurology. 2023. PMID: 37268434 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical