

Clinical outcomes of de novo metastatic HER2-positive inflammatory breast cancer
- PMID: 37268625
- PMCID: PMC10238481
- DOI: 10.1038/s41523-023-00555-w
Clinical outcomes of de novo metastatic HER2-positive inflammatory breast cancer
Abstract
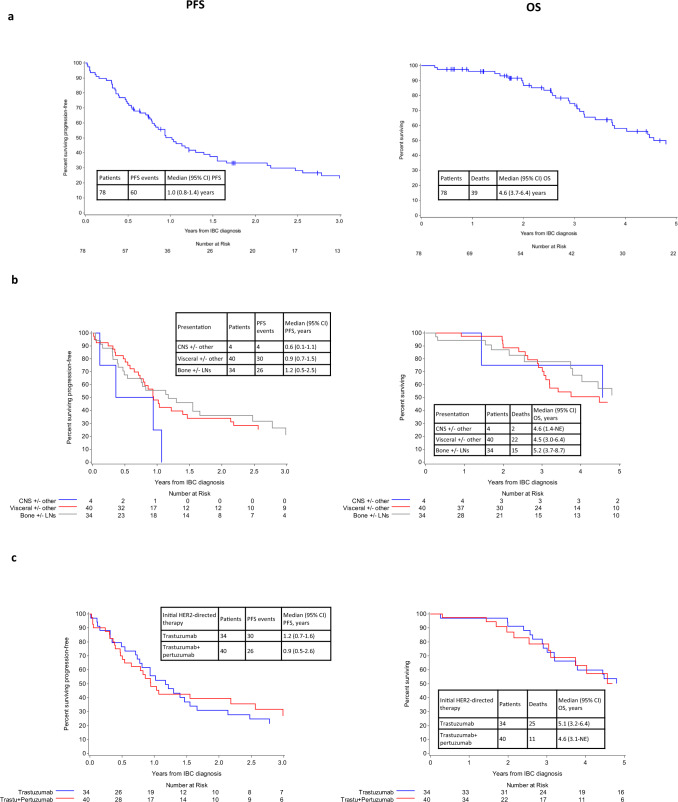
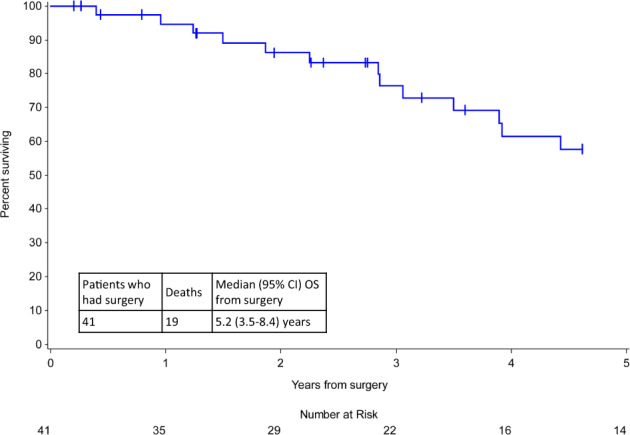
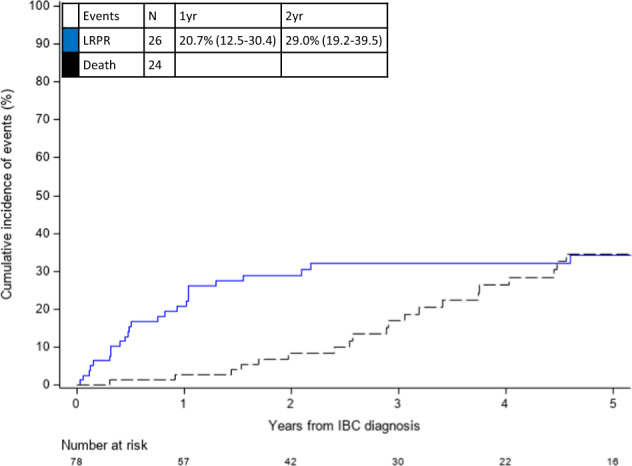
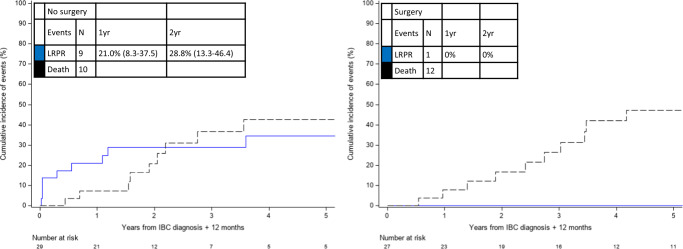
Inflammatory breast cancer (IBC) is a rare, aggressive form of breast cancer that presents as de novo metastatic disease in 20-30% of cases, with one-third of cases demonstrating HER2-positivity. There has been limited investigation into locoregional therapy utilization following HER2-directed systemic therapy for these patients, and their locoregional progression or recurrence (LRPR) and survival outcomes. Patients with de novo HER2-positive metastatic IBC (mIBC) were identified from an IRB-approved IBC registry at Dana-Farber Cancer Institute. Clinical, pathology, and treatment data were abstracted. Rates of LRPR, progression-free survival (PFS), overall survival (OS), and pathologic complete response (pCR) were determined. Seventy-eight patients diagnosed between 1998 and 2019 were identified. First-line systemic therapy comprised chemotherapy for most patients (97.4%) and HER2-directed therapy for all patients (trastuzumab [47.4%]; trastuzumab+pertuzumab [51.3%]; or trastuzumab emtansine [1.3%]). At a median follow-up of 2.7 years, the median PFS was 1.0 year, and the median OS was 4.6 years. The 1- and 2-year cumulative incidence of LRPR was 20.7% and 29.0%, respectively. Mastectomy was performed after systemic therapy in 41/78 patients (52.6%); 10 had a pCR (24.4%) and all were alive at last follow-up (1.3-8.9 years after surgery). Among 56 patients who were alive and LRPR-free at one year, 10 developed LRPR (surgery group = 1; no-surgery group = 9). In conclusion, patients with de novo HER2-positive mIBC who undergo surgery have favorable outcomes. More than half of patients received systemic and local therapy with good locoregional control and prolonged survival, suggesting a potential role for local therapy.
© 2023. The Author(s).
Conflict of interest statement
The authors report the following potential financial competing interests: Consulting/Advising Role: Novartis (S.M.T.), Pfizer (S.M.T., F.L.), Merck (S.M.T.), Eli Lilly and Company (S.M.T.), Nektar Therapeutics (S.M.T.), NanoString Technologies (S.M.T.), AstraZeneca (S.M.T., M.M.R., N.U.L., F.L.), Puma Biotechnology (S.M.T., N.U.L.), Genentech/Roche (S.M.T.), Eisai (S.M.T.), Sanofi (S.M.T.), Bristol Myers Squibb (S.M.T., M.M.R.), Seattle Genetics (S.M.T., N.U.L.), Odonate Therapeutics (S.M.T.), OncoPep (S.M.T.), Kyowa Hakko Kirin (S.M.T.), Samsung Bioepis (S.M.T.), CytomX Therapeutics (S.M.T., F.L.), Daiichi Sankyo (S.M.T., N.U.L., F.L.), Athenex (S.M.T.), Gilead Sciences (S.M.T.), Mersana (S.M.T.), Certara (S.M.T.), Chugai Pharma (S.M.T.), Ellipses Pharma (S.M.T.), Infinity (S.M.T.), 4D Pharma (S.M.T.), OncoSec Medical Inc. (S.M.T.), BeyondSpring Pharmaceuticals (S.M.T.), OncXerna (S.M.T.), Zymeworks (S.M.T.), Zentalis (S.M.T.), Blueprint Medicines (S.M.T.), Reveal Genomics (S.M.T.), ARC Therapeutics (S.M.T.), Ipsen Biopharmaceuticals (M.M.R.), DebioPharm (M.M.R.), Tolmar Pharmaceuticals (M.M.R.), Denali Therapeutics (N.U.L.), Prelude Therapeutics (N.U.L.), Olema Pharmaceuticals (N.U.L.), Aleta BioPharma (N.U.L.), Affinia Therapeutics (N.U.L.), Voyager Therapeutics (N.U.L.), Janssen (N.U.L.), Blueprint Medicines (N.U.L.), OncoSec Medical, Inc. (FL).
Figures
References
-
- Schlichting JA, Soliman AS, Schairer C, Schottenfeld D, Merajver SD. Inflammatory and non-inflammatory breast cancer survival by socioeconomic position in the Surveillance, Epidemiology, and End Results database, 1990-2008. Breast Cancer Res. Treat. 2012;134:1257–1268. doi: 10.1007/s10549-012-2133-2. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
