

Irritable bowel syndrome and mental health comorbidity - approach to multidisciplinary management
- PMID: 37268741
- PMCID: PMC10237074
- DOI: 10.1038/s41575-023-00794-z
Irritable bowel syndrome and mental health comorbidity - approach to multidisciplinary management
Abstract
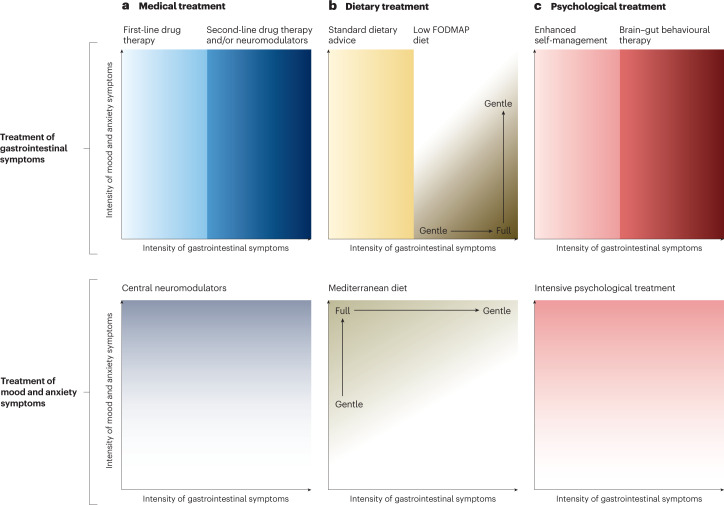
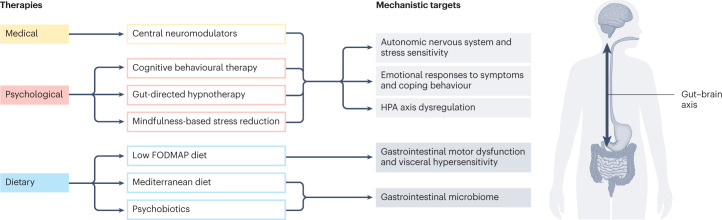
Irritable bowel syndrome (IBS) affects 5-10% of the global population. Up to one-third of people with IBS also experience anxiety or depression. Gastrointestinal and psychological symptoms both drive health-care use in people with IBS, but psychological comorbidity seems to be more important for long-term quality of life. An integrated care approach that addresses gastrointestinal symptoms with nutrition and brain-gut behaviour therapies is considered the gold standard. However, best practice for the treatment of individuals with IBS who have a comorbid psychological condition is unclear. Given the rising prevalence of mental health disorders, discussion of the challenges of implementing therapy for people with IBS and anxiety and depression is critical. In this Review, we draw upon our expertise in gastroenterology, nutrition science and psychology to highlight common challenges that arise when managing patients with IBS and co-occurring anxiety and depression, and provide recommendations for tailoring clinical assessment and treatment. We provide best practice recommendations, including dietary and behavioural interventions that could be applied by non-specialists and clinicians working outside an integrated care model.
© 2023. Springer Nature Limited.
Conflict of interest statement
H.M.S. has received research funding from DSM Pharmaceuticals, the Rome Foundation, VSL Pharmaceuticals; non-financial support from VSL Pharmaceuticals; and consulting fees from Dietitian Connection, Dietitians Australia and Microba. S.B.T. is employed by the University of New South Wales, Sydney, Australia, with funding from the Mindgardens Neuroscience Network; was a contractor to Nutrition Research Australia (2020–2021); and has received consulting fees from the British Dietetic Association, Dietitian Connection, Dietitians Australia, Education in Nutrition, the Royal Australian and New Zealand College of Psychiatrists (Tasmania Branch), the University of Newcastle, Australia, and the University of Technology Sydney, Australia. L.K. is a co-founder, consultant and equity owner in Trellus Health; is a paid consultant for Abbvie, Eli Lilly and Takeda; and serves as a member of the Rome Foundation Board of Directors. The other authors declare no competing interests.
Figures
References
-
- Lacy BE, et al. Bowel disorders. Gastroenterology. 2016;150:1393–1407. doi: 10.1053/j.gastro.2016.02.031. - DOI
-
- World Health Organization. Integrated care models: an overview. WHOhttps://www.researchgate.net/profile/Altynai-Satylganova/publication/315... (2016).
-
- World Health Organization. Depression and other common mental disorders: global health estimates. WHOhttps://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017... (2017).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
