

Neurodegenerative pathologies associated with behavioral and psychological symptoms of dementia in a community-based autopsy cohort
- PMID: 37269007
- PMCID: PMC10236713
- DOI: 10.1186/s40478-023-01576-z
Neurodegenerative pathologies associated with behavioral and psychological symptoms of dementia in a community-based autopsy cohort
Abstract
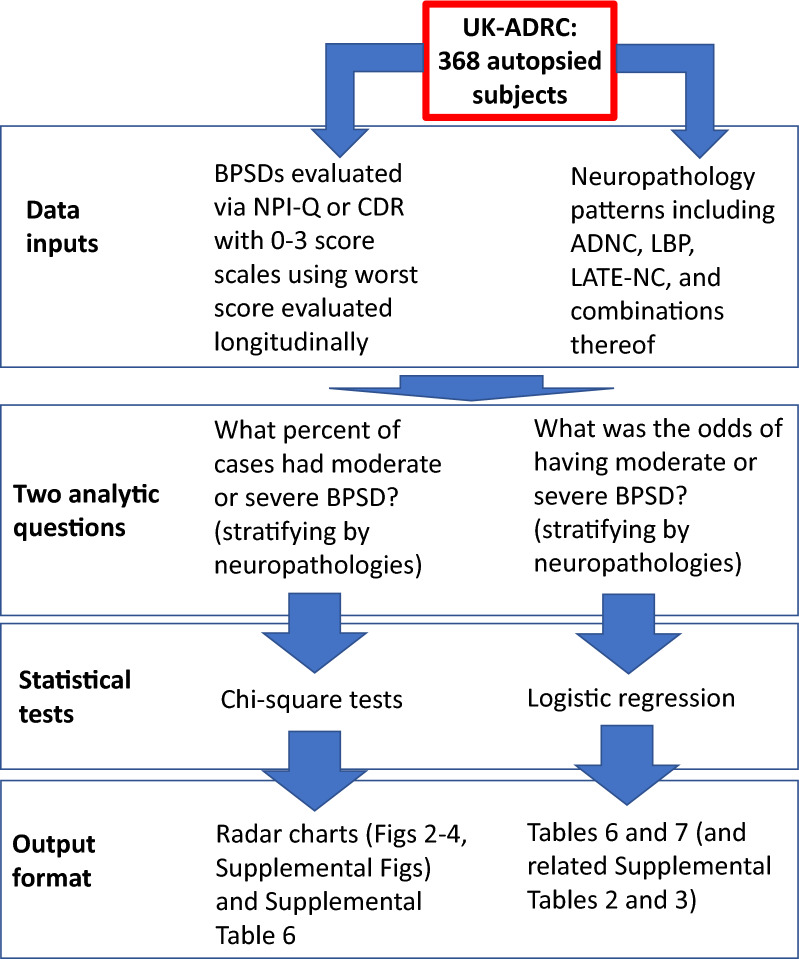
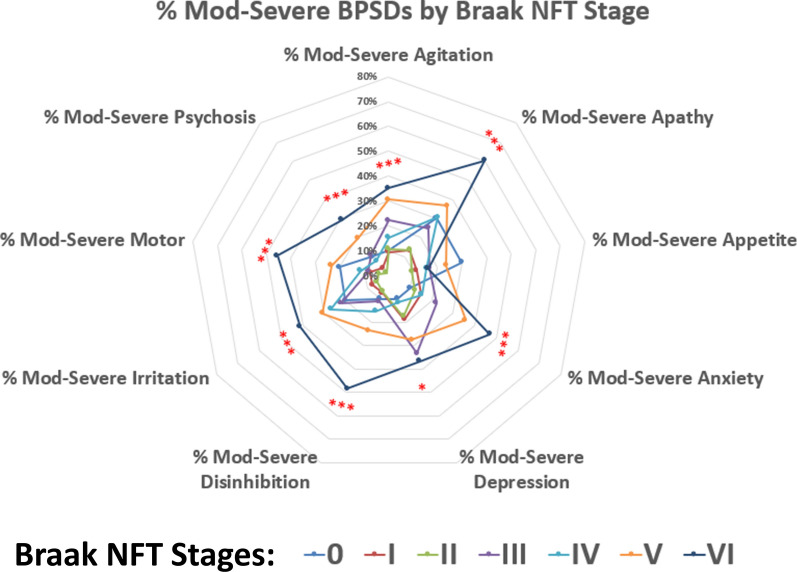
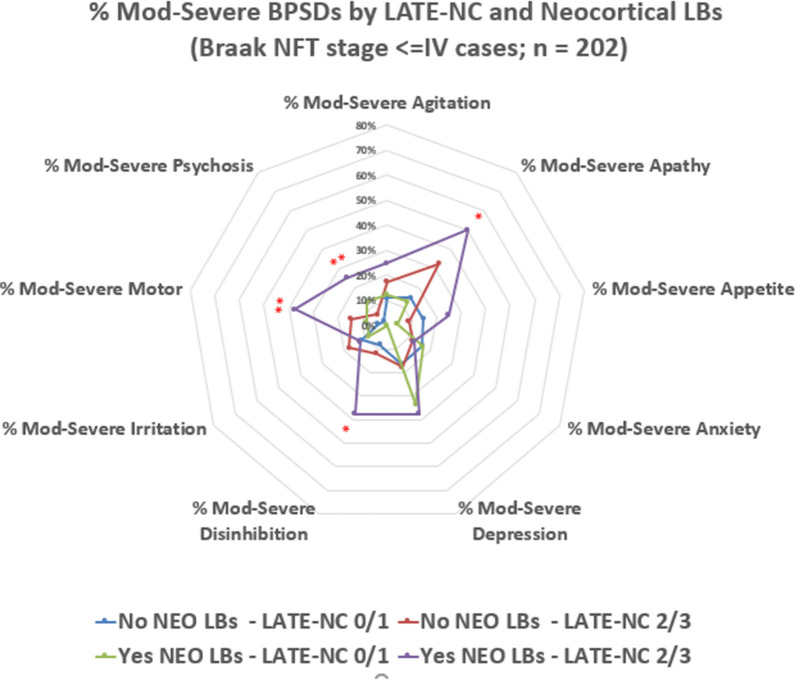
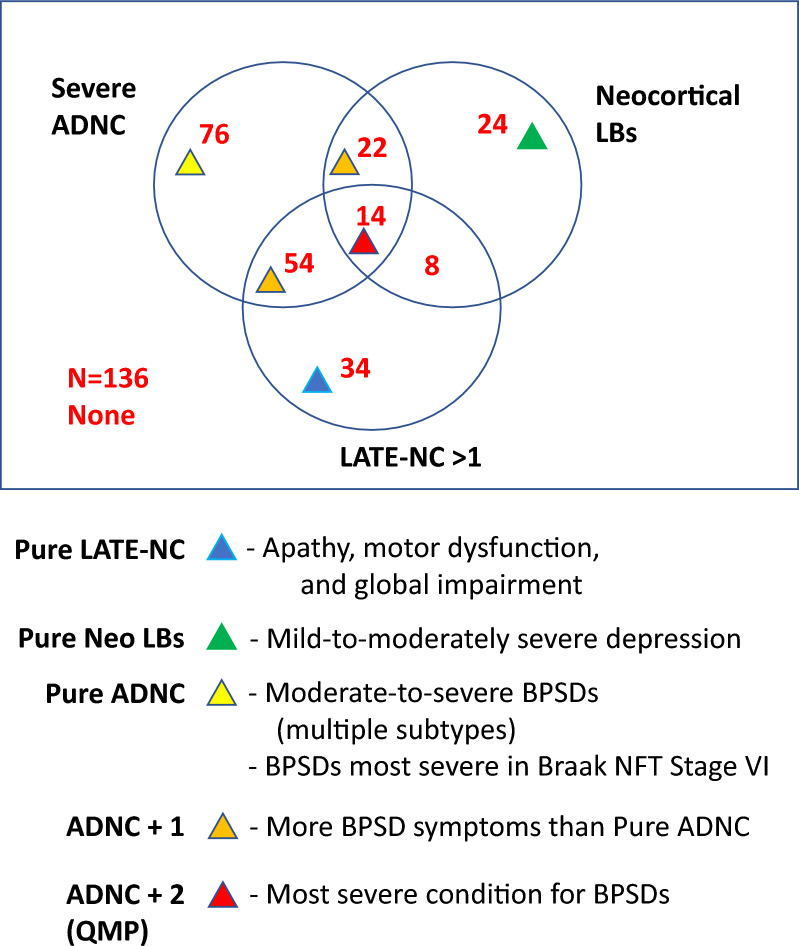
In addition to the memory disorders and global cognitive impairment that accompany neurodegenerative diseases, behavioral and psychological symptoms of dementia (BPSD) commonly impair quality of life and complicate clinical management. To investigate clinical-pathological correlations of BPSD, we analyzed data from autopsied participants from the community-based University of Kentucky Alzheimer's Disease Research Center longitudinal cohort (n = 368 research volunteers met inclusion criteria, average age at death 85.4 years). Data assessing BPSD were obtained approximately annually, including parameters for agitation, anxiety, apathy, appetite problems, delusions, depression, disinhibition, hallucinations, motor disturbance, and irritability. Each BPSD was scored on a severity scale (0-3) via the Neuropsychiatric Inventory Questionnaire (NPI-Q). Further, Clinical Dementia Rating (CDR)-Global and -Language evaluations (also scored on 0-3 scales) were used to indicate the degree of global cognitive and language impairment. The NPI-Q and CDR ratings were correlated with neuropathology findings at autopsy: Alzheimer's disease neuropathological changes (ADNC), neocortical and amygdala-only Lewy bodies (LBs), limbic predominant age-related TDP-43 encephalopathy neuropathologic changes (LATE-NC), primary age-related tauopathy (PART), hippocampal sclerosis, and cerebrovascular pathologies. Combinations of pathologies included the quadruple misfolding proteinopathy (QMP) phenotype with co-occurring ADNC, neocortical LBs, and LATE-NC. Statistical models were used to estimate the associations between BPSD subtypes and pathologic patterns. Individuals with severe ADNC (particularly those with Braak NFT stage VI) had more BPSD, and the QMP phenotype was associated with the highest mean number of BPSD symptoms: > 8 different BPSD subtypes per individual. Disinhibition and language problems were common in persons with severe ADNC but were not specific to any pathology. "Pure" LATE-NC was associated with global cognitive impairment, apathy, and motor disturbance, but again, these were not specific associations. In summary, Braak NFT stage VI ADNC was strongly associated with BPSD, but no tested BPSD subtype was a robust indicator of any particular "pure" or mixed pathological combination.
Keywords: Aphasia; FTD; FTLD; HS-aging; Psychiatric; Psychoses; Psychosis; Synuclein; Tau; Tauopathy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
The association of Lewy bodies with limbic-predominant age-related TDP-43 encephalopathy neuropathologic changes and their role in cognition and Alzheimer's dementia in older persons.Acta Neuropathol Commun. 2021 Sep 25;9(1):156. doi: 10.1186/s40478-021-01260-0. Acta Neuropathol Commun. 2021. PMID: 34563269 Free PMC article.
-
Disentangling and quantifying the relative cognitive impact of concurrent mixed neurodegenerative pathologies.Acta Neuropathol. 2024 Mar 23;147(1):58. doi: 10.1007/s00401-024-02716-y. Acta Neuropathol. 2024. PMID: 38520489 Free PMC article.
-
Neuropsychiatric symptoms in limbic-predominant age-related TDP-43 encephalopathy and Alzheimer's disease.Brain. 2020 Dec 1;143(12):3842-3849. doi: 10.1093/brain/awaa315. Brain. 2020. PMID: 33188391 Free PMC article.
-
Investigating neuropathological correlates of hyperactive and psychotic symptoms in dementia: a systematic review.Front Dement. 2025 Jan 29;4:1513644. doi: 10.3389/frdem.2025.1513644. eCollection 2025. Front Dement. 2025. PMID: 39949536 Free PMC article.
-
Revisiting the cholinergic hypothesis of behavioral and psychological symptoms in dementia of the Alzheimer's type.Ageing Res Rev. 2011 Sep;10(4):404-12. doi: 10.1016/j.arr.2011.01.003. Epub 2011 Feb 1. Ageing Res Rev. 2011. PMID: 21292041 Review.
Cited by
-
Alcohol Use Disorder and Dementia: A Review.Alcohol Res. 2024 May 23;44(1):03. doi: 10.35946/arcr.v44.1.03. eCollection 2024. Alcohol Res. 2024. PMID: 38812709 Free PMC article. Review.
-
Practical Assessment of Neuropsychiatric Symptoms: Updated Reliability, Validity, and Cutoffs for the Neuropsychiatric Inventory Questionnaire.Am J Geriatr Psychiatry. 2025 May;33(5):524-534. doi: 10.1016/j.jagp.2024.10.014. Epub 2024 Oct 28. Am J Geriatr Psychiatry. 2025. PMID: 39551647
-
Plasma phosphorylated tau and neuropsychiatric symptoms in dementia with Lewy bodies.Alzheimers Dement. 2025 Feb;21(2):e14434. doi: 10.1002/alz.14434. Epub 2024 Dec 28. Alzheimers Dement. 2025. PMID: 39732510 Free PMC article.
-
Clinical criteria for limbic-predominant age-related TDP-43 encephalopathy.Alzheimers Dement. 2025 Jan;21(1):e14202. doi: 10.1002/alz.14202. Epub 2025 Jan 14. Alzheimers Dement. 2025. PMID: 39807681 Free PMC article.
-
Exploring the link between dystrophic microglia and the spread of Alzheimer's neuropathology.Brain. 2025 Jan 7;148(1):89-101. doi: 10.1093/brain/awae258. Brain. 2025. PMID: 39101580 Free PMC article.
References
-
- Abner EL, Neltner JH, Jicha GA, Patel E, Anderson SL, Wilcock DM, Van Eldik LJ, Nelson PT. Diffuse amyloid-beta plaques, neurofibrillary tangles, and the impact of APOE in elderly persons' brains lacking neuritic amyloid plaques. J Alzheimers Dis. 2018;64:1307–1324. doi: 10.3233/JAD-180514. - DOI - PMC - PubMed
-
- Attems J, Toledo JB, Walker L, Gelpi E, Gentleman S, Halliday G, Hortobagyi T, Jellinger K, Kovacs GG, Lee EB, et al. Neuropathological consensus criteria for the evaluation of Lewy pathology in post-mortem brains: a multi-centre study. Acta Neuropathol. 2021;141:159–172. doi: 10.1007/s00401-020-02255-2. - DOI - PMC - PubMed
-
- Bachstetter AD, Van Eldik LJ, Schmitt FA, Neltner JH, Ighodaro ET, Webster SJ, Patel E, Abner EL, Kryscio RJ, Nelson PT. Disease-related microglia heterogeneity in the hippocampus of Alzheimer’s disease, dementia with Lewy bodies, and hippocampal sclerosis of aging. Acta Neuropathol Commun. 2015;3:32. doi: 10.1186/s40478-015-0209-z. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
